The U.K. National Institute for Clinical Excellence (NICE) published its long-awaited update to the chest pain guidelines on 30 November, with leading cardiac imaging specialists issuing a positive, but cautious, response to the new document.
For patients without known significant coronary artery disease, the NICE statement supports coronary CT angiography (CCTA) as the first-line investigation for all patients who present with typical and atypical angina. It recommends functional imaging or invasive angiography as a second-line investigation in those cases where CCTA is equivocal or positive.
"Whilst the increased use of CT coronary angiography is very much welcomed, the delivery of these guidelines represent a significant challenge in the U.K., even for well-established, high-volume cardiac CT centers," noted Dr. Ed Nicol, president of the British Society of Cardiovascular Imaging (BSCI) and British Society of Cardiovascular CT (BSCCT), in a response designed to provide a delivery perspective.
According to Nicol, who is also honorary consultant cardiologist and honorary senior lecturer at the Royal Brompton Hospital and National Heart and Lung Institute, Imperial College in London, the key points made in the NICE update are the following:
- Include the typicality of anginal pain features in all requests for diagnostic investigations and in the patient's notes.
- Use clinical judgement and take into account people's preferences and comorbidities when considering diagnostic testing.
- Offer 64‑slice (or above) CCTA if clinical assessment indicates typical or atypical angina, or if clinical assessment indicates nonanginal chest pain but 12‑lead resting ECG has been done and indicates ST‑T changes or Q waves.
- For people with confirmed coronary artery disease (e.g., previous myocardial infarction, revascularization, previous angiography), offer noninvasive functional testing when there is uncertainty about whether chest pain is caused by myocardial ischemia. An exercise ECG may be used instead of functional imaging.
The two cases below help to show two distinct types of patients who should be served well by the new guidelines, said Dr. John G. Dreisbach, specialist trainee (ST5) in clinical radiology at Glasgow Royal Infirmary, U.K., who assisted with the data-gathering work for the BSCI-BSCCT response.
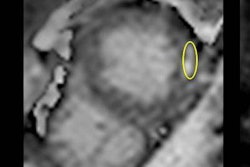
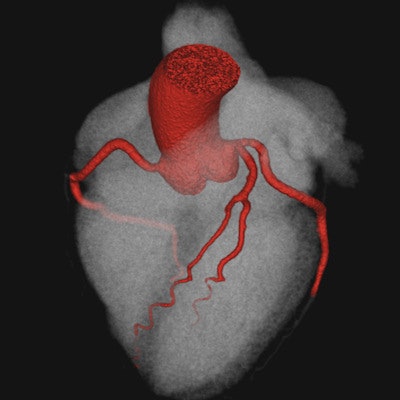
 A 68-year-old man with a history of hypertension was reviewed at a rapid access chest pain clinic in January 2016 with atypical nonexertional central chest pain. An exercise tolerance test lasting under seven minutes elicited no chest pain but did demonstrate inferolateral ST depression. CCTA performed in March 2016 demonstrated severe stenosis in the proximal left anterior descending artery (LAD) due to a 10 mm long segment of mixed morphology plaque. The patient underwent elective percutaneous cardiac intervention in May with catheter angiography confirming 90% stenosis in the proximal LAD, which was treated with a drug-eluting stent with a satisfactory angiographic result. The patient made a good recovery, and on clinical review in June 2016, he reported having more energy with no recurrence of cardiac symptoms. Top: 3D reconstruction overview of the coronary arteries. Below: LAD lesion due to mixed morphology plaque, causing severe stenosis, shown on CCTA. Final image left: Catheter angiography confirming 90% stenosis in the LAD. Final image right: Catheter angiography after stent showing good result. All images courtesy of Dr. John G. Dreisbach.
A 68-year-old man with a history of hypertension was reviewed at a rapid access chest pain clinic in January 2016 with atypical nonexertional central chest pain. An exercise tolerance test lasting under seven minutes elicited no chest pain but did demonstrate inferolateral ST depression. CCTA performed in March 2016 demonstrated severe stenosis in the proximal left anterior descending artery (LAD) due to a 10 mm long segment of mixed morphology plaque. The patient underwent elective percutaneous cardiac intervention in May with catheter angiography confirming 90% stenosis in the proximal LAD, which was treated with a drug-eluting stent with a satisfactory angiographic result. The patient made a good recovery, and on clinical review in June 2016, he reported having more energy with no recurrence of cardiac symptoms. Top: 3D reconstruction overview of the coronary arteries. Below: LAD lesion due to mixed morphology plaque, causing severe stenosis, shown on CCTA. Final image left: Catheter angiography confirming 90% stenosis in the LAD. Final image right: Catheter angiography after stent showing good result. All images courtesy of Dr. John G. Dreisbach.CCTA is a relatively new technique, so the number of professionals currently trained in its acquisition and reporting is limited, and modern equipment is essential for high-quality, low-dose CCTA, pointed out Dr. Huon Gray, national clinical director for heart disease at NHS (National Health Service) England, and Dr. Nicola Strickland, president of the Royal College of Radiologists, in a foreword to the BSCI-BSCCT report. For these reasons, geographic variations exist in the availability and delivery of CCTA services within the U.K., they added.
 A 49-year-old woman with a personal history of hypertension, hypercholesterolemia, and an immediate family history of premature death due to ischemic heart disease was reviewed at a cardiology clinic in December 2015 with recurrent typical chest pain related to exertion and stress. An exercise tolerance test was stopped after five minutes due to dyspnea and elicited no chest pain but did demonstrate exercise-related left bundle branch block. CCTA in April 2016 demonstrated no evidence of coronary artery disease. Top: 3D reconstruction overview of the coronary arteries. Below: Normal LAD. Center: Normal left circumflex artery (LCx). Final image: Normal right coronary artery (RCA).
A 49-year-old woman with a personal history of hypertension, hypercholesterolemia, and an immediate family history of premature death due to ischemic heart disease was reviewed at a cardiology clinic in December 2015 with recurrent typical chest pain related to exertion and stress. An exercise tolerance test was stopped after five minutes due to dyspnea and elicited no chest pain but did demonstrate exercise-related left bundle branch block. CCTA in April 2016 demonstrated no evidence of coronary artery disease. Top: 3D reconstruction overview of the coronary arteries. Below: Normal LAD. Center: Normal left circumflex artery (LCx). Final image: Normal right coronary artery (RCA)."We will be focusing on these guidelines for the foreseeable future and we look forward to working together with our stakeholders and partners to implement them in a way that ensures high-quality care for our patients," Nicol emphasized. "We will also continue to support our members who undertake functional cardiovascular imaging, which clearly remains a core part of the investigation of patients with chest pain."
To read the full NICE guideline, click here.
To download the 13-page BSCI-BSCCT response, click here.