Using BI-RADS to detect ductal carcinoma in situ (DCIS) with MRI results in higher sensitivity and positive predictive value (PPV) than mammography, according to new Brazilian research published in the European Journal of Radiology.
The prospective, observational study included patients who presented with microcalcifications on screening mammography and underwent an MRI exam followed by a biopsy. The study team, led by Dr. Gustavo Machado Badan, a doctoral student in the breast imaging service of the radiology department at Irmandade da Santa Casa de Misericórdia de São Paulo, found the combination of BI-RADS and MRI rivaled mammography (Eur J Radiol, 18 July 2016).
"BI-RADS as a tool for the detection of DCIS by MRI is a powerful instrument whose sensitivity was higher when compared to that observed for mammography in the literature," Badan and colleagues noted.
The complexity of DCIS
DCIS can be hidden in between 6% and 23% of mammography cases. In addition, approximately 75% to 85% of suspicious microcalcifications detected at mammography are deemed benign following biopsy. Obviously, a better detection method is needed, but DCIS is complicated.


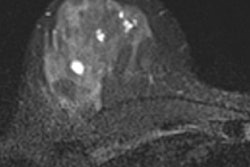
A: Mammograms with digital magnification of side profile view featuring pleomorphoic grouped microcalcifications (highlighted areas) at the left breast at junction of the upper quadrants, BI-RADS category 4B. B: MRI: Axial T1 sequence following administration of contrast agent with image subtraction displays linear and heterogeneous nonmass lesion enhancement (arrow) in the topography of microcalcifications observed on mammogram, BI-RADS category 4C: Histological sections showing solid neoplastic proliferation, increase in nuclear size and restriction to the duct, compatible with intermediate nuclear-grade DCIS. Images courtesy of Dr. Gustavo Machado Badan.
The factors associated with the progression of DCIS to invasive breast cancer are poorly understood. Many studies have focused on the role of the molecular and genetic alterations in neoplastic epithelial cells, but emerging evidence suggests the transition from DCIS to invasive cancer is strongly dependent upon alterations in the microenvironment.
The role of myoepithelial cells, responsible for the synthesis and maintenance of the basal membrane and stromal cells that stimulate tumor growth and stromal angiogenesis, has been emphasized in the literature, and their main presentation is in the form of clustered microcalcifications, according to the authors. However, only 75% of all DCIS cases present with calcifications, and the sensitivity of mammography ranges from 27% to 80%.
"Due to the wide variation in sensitivity rates observed in the literature and to the fact that, as far as we know, there are no studies demonstrating the performance of other BI-RADS indicators in evaluating DCIS by MRI, it is appropriate to verify these indicators in patients participating in a screening program at a teaching hospital," they wrote.
Thus, Badan and colleagues sought to determine the sensitivity, specificity, predictive values, and accuracy of BI-RADS in detecting DCIS by MRI.
MRI's performance
The study lasted for two years and, after weeding out exclusions, consisted of 99 consecutive patients. The women presented with suspicious or highly suspicious microcalcifications on screening mammography (BI-RADS 4 and 5). They underwent stereotactic-guided breast biopsy following breast MRI.
The researchers found 38 cases were positive for malignancy, of which 25 were DCIS and 13 were invasive ductal carcinoma cases.
They determined sensitivity, specificity, and negative predictive value (NPV) for both MRI and mammography, but they also found positive predictive value for mammography. In addition, they compared mammography's sensitivity to that found in other studies.
| MRI plus BI-RADS results | ||||
| Sensitivity | Specificity | PPV | NPV | |
| MRI | 96% | 75.67% | 57.14% | 98.24% |
| Mammography | 27% to 80% | - | 25.25% | - |
"In searching for more accurate indicators, this study aimed to evaluate the BI-RADS indicators in the detection of DCIS by MRI," the authors wrote. "We have observed that MRI is a powerful tool that helps to increase PPV in detecting DCIS from 25.25% by mammography to 57.14% on MRI scans."
The researchers attribute their results to mastering the breast MRI learning curve and the small sample size.
"According to the results we obtained in our study, if the recommendation to conduct a breast biopsy of all 99 cases involving microcalcifications classified as BI-RADS categories 4 and 5 had been based on the MRI findings, due to their high NPV, 57 biopsies could have been avoided," the authors stated.
A high NPV can provide initial evidence that MRI scans can serve as an alternative to the recommendation for a biopsy, but multicenter studies are needed to validate this alternative, they added.
The authors noted that one limitation of this study was that MRI was assessed only in patients with mammographic changes that were classified as suspicious microcalcifications, so noncalcified DCIS lesions were not evaluated, even though they might show enhancement on MRI. Also, the evaluation of the MRI findings may have been influenced by the presence of microcalcifications on the same topography, although the comparative analysis with other diagnostic methods is recommended by the BI-RADS guidelines.
Finally, another limitation was the rather low number of patients, which was caused by the selection of patients with pure DCIS to avoid diagnostic bias due to mixed invasive and carcinoma in situ.
Nonetheless, the data show MRI is a promising method with a high diagnostic accuracy, the researchers concluded.