Symptomatic patients with very low coronary artery calcium scores are almost as likely to have a positive SPECT myocardial perfusion imaging (MPI) scan and a subsequent cardiac event as patients with higher calcium scores, according to a study presented at the Society of Nuclear Medicine and Molecular Imaging (SNMMI) annual meeting.
Researchers at Rambam Health Care Campus in Haifa, Israel, found that approximately one in five symptomatic patients with a calcium score of 10 or less had a positive MPI scan and a coronary event within 12 months.
"In symptomatic patients, a very low coronary artery calcium score alone cannot rule out functionally significant coronary artery disease," lead author Dr. Samia Massalha, a senior cardiologist at Rambam, told SNMMI attendees. "Further and more aggressive management decisions, such as careful follow-up and additional testing, should be considered for patients with positive MPI."
Early signs
Coronary artery calcification can be an early indication of atherosclerosis and often precedes obstructive coronary artery disease by many years. In turn, the absence of coronary artery calcium is associated with a low probability of significant obstruction.
In either case, the clinical consensus is to recommend coronary artery calcium scoring in symptomatic patients prior to coronary angiography to gauge the extent of a patient's condition.
Massalha cited past papers that calculated calcium score in some 9,000 symptomatic patients, using coronary angiography as the gold standard, to suggest that a coronary artery calcium score of 0 means there is no obstructive coronary artery disease, with a negative predictive value as great as 97%.
However, other studies indicate that between 2% and 8% of patients with no calcification may still have luminal stenosis as seen on CT angiography. This condition is mostly associated with young symptomatic patients and smokers.
Case study
As an example of the exceptions to the norm, Massalha presented the case of a 42-year-old woman with no significant past medical history or cardiovascular risk factors, except for hyperlipidemia, which was treated with statins. The patient presented to a cardiologist with chest pain, and her exercise stress test was inconclusive. Her baseline electrocardiogram (ECG) was normal, so she was referred for an MPI study.
"The protocol in our institution is to perform combined MPI and calcium scores for each patient with no known previous cardiovascular disease," Massalha explained.
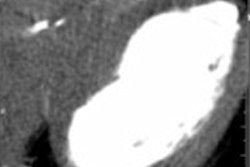
Clinicians came to discover that the woman had a calcium score of 0, but her MPI showed a perfusion defect in the left anterior descending (LAD)-apex and in the anterior apical region. She was referred to the cath lab for the occlusion in her LAD and eventually underwent coronary artery bypass grafting (CABG).
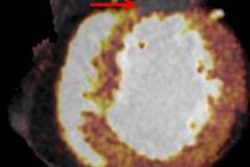
 SPECT MPI study is positive for ischemia in a woman with a very low calcium score, no signs of ischemia in her ECG, and no previous myocardial infarction. Image courtesy of Dr. Samia Massalha.
SPECT MPI study is positive for ischemia in a woman with a very low calcium score, no signs of ischemia in her ECG, and no previous myocardial infarction. Image courtesy of Dr. Samia Massalha.The purpose of the study presented at SNMMI was to determine the value of combined MPI and calcium score in the diagnosis and risk stratification of symptomatic patients with suspected coronary artery disease by examining a larger patient population.
During 2014, Massalha and colleagues enrolled 1,756 symptomatic patients with no previously known coronary artery disease, performed SPECT MPI studies, and calculated each subject's calcium score.
MPI was performed using same-day rest and stress studies, with 296 MBq of technetium-99m MIBI for rest and 926 MBq for stress. All studies were conducted on a SPECT/CT system with cadmium zinc telluride detectors and a 64-detector-row CT module (Discovery NM/CT 570c, GE Healthcare). CT was used for attenuation correction and to perform calcium score measurements (SmartScore software, GE).
"Our specific interest was with patients with a calcium score of less than 100," Massalha said.
Those patients were divided into two groups: Group A, the primary study group, included 517 symptomatic patients with a median age of 56 years (range: 32-81 years) and calcium scores of 10 or less. Group B, the control group, consisted of 367 patients with calcium scores of 11 to 99 and a median age of 61 years (range: 34-76 years).
Patient follow-up
All patients with positive MPI results and calcium scores of less than 100 were followed for 12 months. The end points for follow-up were based on myocardial infarction, hospitalization for unstable angina, and coronary revascularization.
"We also recorded the presence of significant coronary artery disease, defined as luminal stenosis greater than 50%, in patients who underwent either invasive or noninvasive CT coronary angiography," Massalha said.
Their analysis revealed that 32 patients (6%) in main study group had positive MPI results, despite very low calcium scores between 0 and 10. Of those subjects, 10 (31%) needed coronary angiography, and nine (90%) of the 10 had significant coronary artery disease. Of those nine individuals, six required revascularization.
Within the control group, 41 patients (11%) had positive MPI results. Of those patients, 22 (54%) required coronary angiography, and 15 (68%) of the 22 had significant coronary artery disease. Ten of the 15 individuals required revascularization, and one had a myocardial infarction.
The key finding is that six (19%) of the 32 patients with very low calcium scores and a positive MPI had a follow-up coronary revascularization, compared with 11 (27%) of the 41 patients in the control group who had higher calcium scores and a positive MPI and underwent revascularization or treatment for a heart attack.
"Therefore, in symptomatic patients, a very low coronary artery calcium score alone cannot rule out functionally significant coronary artery disease," Massalha reiterated. "Our suggestion is that for every clinically suspected patient, no matter how low calcium score is, an MPI should be performed."
Taking the findings one step further, Massalha questioned whether soft plaque is to blame for the need for additional treatment in patients with very low calcium scores.
"Several studies have demonstrated that calcium score measurements have a lower sensitivity in patients younger than 40 or 45 years of age, which was not part of our patient population," she added. "The identification of noncalcified plaque may very well be a plaque at an earlier stage of atherosclerosis."