When it comes to ovarian tumors, MRI is an essential problem-solving tool because it's so efficient at detecting, characterizing, and staging adnexal masses and can have a major impact on patient management, according to a new Italian study.
The researchers have evaluated epidemiology, etiopathogenesis, classification, staging, and diagnostic approaches to ovarian masses and propose an MRI-guided approach to the differential diagnosis of ovarian tumors based on morphological appearance. They also describe MR signal intensity features and enhancement behavior of each lesion using pathologically proven examples from their institution (Insights into Imaging, 16 December 2015).
"The main advantages of MRI are the high contrast resolution and lack of ionizing radiation exposure," noted lead author Dr. Pietro Valerio Foti from the Radiodiagnostic and Radiotherapy Unit at University Hospital Policlinico-Vittorio Emanuele in Catania. "Although different pathological conditions may show similar radiologic manifestations, radiologists should be aware of MRI features of ovarian lesions that may orientate differential diagnosis."
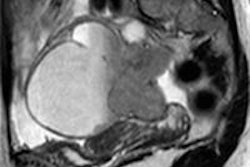
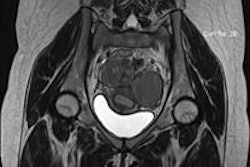
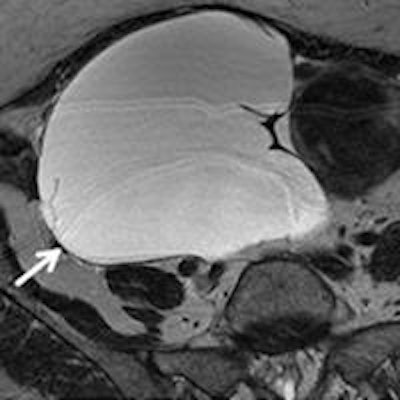
 Serous cystadenoma in a 64-year-old woman. (a) Sagittal and (b) axial T2-weighted images show a hyperintense unilocular cystic mass (white arrows). On (c) sagittal and (d) axial contrast-enhanced fat-suppressed T1-weighted images, the cyst wall shows poor contrast enhancement (white arrows) without vegetations, nodularity, or solid components. All images courtesy of Dr. Pietro Valerio Foti.
Serous cystadenoma in a 64-year-old woman. (a) Sagittal and (b) axial T2-weighted images show a hyperintense unilocular cystic mass (white arrows). On (c) sagittal and (d) axial contrast-enhanced fat-suppressed T1-weighted images, the cyst wall shows poor contrast enhancement (white arrows) without vegetations, nodularity, or solid components. All images courtesy of Dr. Pietro Valerio Foti.Ovarian masses are a common finding in daily clinical practice and may be incidentally detected or identified in symptomatic patients, according to the researchers. Characterization of an ovarian lesion represents a diagnostic challenge: it is of great importance in the preoperative setting to plan adequate therapeutic procedures and may influence patient's management.
MRI can provide useful information for the characterization of ovarian masses as non-neoplastic or neoplastic, and, in the latter case, as benign or malignant, thus radiologists play an important role in the multidisciplinary approach of an ovarian mass. Different pathological conditions may have similar radiologic manifestations, so radiologists should be aware of MRI features of ovarian lesions that may orientate the differential diagnosis.
The MR imaging protocol the researchers used to study patients with ovarian masses was imaging in a closed-configuration superconducting 1.5-tesla system (Signa HDxT, GE Healthcare) with 57.2 mT/m gradient strength and 120 T/m/sec slew rate, by using an eight-channel high-resolution torso coil with array spatial sensitivity technique (ASSET) parallel acquisition.
In their research, Foti and colleagues found morphological characteristics of adnexal masses range from cystic (both unilocular and multilocular), to complex (cystic and solid), to predominantly solid.
"[T]here is a certain overlap between benign and malignant tumors; in particular, it has to be considered that borderline lesions are very difficult to differentiate because they have both benign and malignant features," they wrote.
The most predictive characteristics of malignancy are vegetations in a cystic lesion, presence of ascites, a maximal diameter greater than 6 cm, and necrosis in a solid lesion. Other research suggests malignancy in the demonstration of solid, solid/cystic enhancing masses (greater than 4 cm in maximum diameter) with papillary projections, and irregular thick wall and septa (greater than 3 mm) into a cystic lesion, as well as a heterogeneous and early enhancement pattern.
Key imaging features
The authors found some key imaging features and offer general advice that could help in determining the differential diagnosis of adnexal masses:
- Non-neoplastic lesions should always be taken into consideration.
- In a patient with endometriosis, the presence of a complex and rapidly growing mass with contrast enhancement should raise the suspicion of endometrioid or clear cell tumor.
- A very low signal intensity on T2-weighted images indicates a fibrotic component, suggesting a tumor of the coma/fibroma group, a cystadenofibroma, or a Brenner tumor.
- Sequences with fat saturation are helpful when facing a mass with high signal intensity on T1-weighted images, because the signal suppression is suggestive of a teratoma; otherwise, an endometrial cyst or other hemorrhagic lesion should be considered.
- A stained-glass appearance with cystic loculi of variable signal intensity usually refers to a mucinous tumor because of the different mucin concentration.
- Metastasis should be considered if a complex, enhancing mass is demonstrated in both ovaries (eventually looking for an unknown primary tumor).
- Remember serous epithelial tumors can be bilateral as well.