Hereditary syndromes are responsible for about 10% of gynecologic cancers, but are there any distinctive imaging features that accompany them? Unfortunately not, Portuguese researchers have found, but they have identified other key points.
The researchers Dr. Nelson Neto from the radiology department at Centro Hospitalar de Lisboa Ocidental and Dr. Teresa Margarida Cunha from the radiology department at Instituto Português de Oncologia de Lisboa Francisco Gentil, in Lisbon, were keen to provide an updated perspective on the evidence-based specific features of tumors related to certain hereditary syndromes and also on the most accepted screening and surveillance guidelines.
"It was quite disappointing for us as radiologists to verify that apparently there are no distinctive imaging features of these cancers, and, thus, we might only suggest further investigation based on clinical information provided and/or pathology reports in case none of the other clinicians still haven't raised suspicion," he noted in an email to AuntMinnieEurope.com.
What they learned
According to the American Society of Clinical Oncology (ASCO), hereditary syndromes account for about 10% of gynecologic cancers such as the association between germ line mutations in breast cancer (BRCA) 1 and 2 genes and ovarian cancers in hereditary breast-ovarian cancer syndrome.

Despite the evidence of these inherited disorders' susceptibility to gynecologic cancers, it is still unclear whether these tumors have any epidemiologic, clinical, pathologic, or imaging specific features that could allow any of the intervening physicians to raise suspicion of a hereditary syndrome in patients without known genetic risk, the authors wrote (Insights into Imaging, 4 September 2015). Also, their screening and surveillance schemes remain controversial.
"At first, as regular participants in multidisciplinary consultation in the field of gynecologic cancer, we got curious if any of the participants (gynecologists, oncologists, pathologists, and radiologists) could be able to identify families with genetic risk among the general population," Neto noted in his email. "Basically we wondered if there were any clues, other than the family history, for us to depict and give our own contribution."
They didn't find many clues, but did make other findings:
- Hereditary breast-ovarian cancer syndrome is mainly associated with ovarian high-grade serous carcinomas, which seem to arise in the fallopian fimbriae and have better prognosis than sporadic cancers.
- Lynch syndrome predisposes a patient to endometrial cancer, at a lower rate than ovarian cancers. Endometrial cancers show a predilection for the lower uterine segment and tend to be histologically more diverse in contrast to their sporadic counterparts, including nonendometrioid carcinomas. Ovarian cancers related to Lynch syndrome and Cowden syndrome are mostly of the nonserous type, usually endometrioid.
- Li-Fraumeni syndrome only slightly increases the risk of endometrial and ovarian cancers.
- Peutz-Jeghers syndrome increases the risk of ovarian, cervical, and uterine cancers, in decreasing order, and also ovarian sex cord tumors with annular tubules and cervical adenoma malignum being strongly associated.
- To ensure early identification of high-risk patients, every time a gynecologic malignancy is diagnosed under the expected age in the general population, a careful anamnesis that includes familial history of cancer and genetic confirmation when indicated is required.
- Screening and surveillance schemes usually consist of an annual pelvic examination with endometrial sampling and ultrasound, beginning in young adulthood.
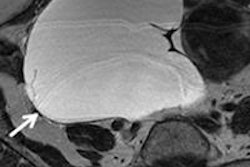
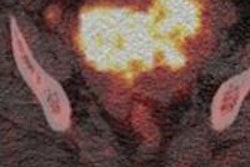
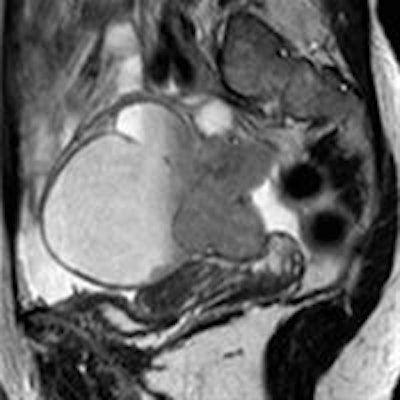
 Undifferentiated ovarian carcinoma in a 59-year-old woman who is a carrier of the BRCA2 mutation. CT demonstrates a large, multilobulated complex cystic-solid right adnexal mass. There were neither ascites nor enlarged lymph nodes.
Undifferentiated ovarian carcinoma in a 59-year-old woman who is a carrier of the BRCA2 mutation. CT demonstrates a large, multilobulated complex cystic-solid right adnexal mass. There were neither ascites nor enlarged lymph nodes.Turning lemons into lemonade
Despite the slight disappointment, some good has come out of the research.
"We've presented the results of our literature review to the other members of the multidisciplinary team in order to make them beware of some particularities and associations we've found for each syndrome, some of which were unknown to them. So, it was somehow useful," Neto said.
Neto and colleagues aren't planning any additional studies in the topic of hereditary syndromes due to the fact there does not seem to be any specific imaging features, but of course they'll remain available to make contributions to future investigations together with other medical specialties, they said.