CT use in pregnant women is climbing, but are good clinical practices being followed, especially when it comes to radiation dose? The answer is mostly yes, at least at one Belgian hospital, which found that radiation dose met guidelines despite a threefold increase in scans in the last few years.
Researchers conducted a retrospective review of all CT exams performed in pregnant patients from 2008 to 2013 that took place at University Hospitals Leuven in Belgium. The team led by Dr. Sofie Woussen from the hospital's radiology department compared estimated radiation doses to the fetus in early stages of pregnancy with published data (European Radiology, 23 July 2015).
The researchers found most clinical indications and doses were in line with good clinical practice -- only two cases delivered radiation dose higher than 50 mGy. As a result of the audit, the researchers seek to establish internal guidelines for the appropriate use of imaging during pregnancy at their department.
"All our conceptus [early-stage fetus] dose estimates except for two polytrauma CT examinations were lower than or similar to the highest dose values found in the literature," Woussen and colleagues wrote. "Three pregnancies were accidentally discovered on CT. The rest of the indications were examples of good clinical practice."
 CT exam of a patient with Crohn's disease, pregnant for six weeks and previously unknown. All images courtesy of Dr. Federica Zanca.
CT exam of a patient with Crohn's disease, pregnant for six weeks and previously unknown. All images courtesy of Dr. Federica Zanca.CT for pregnant patients is concerning
CT use is on the rise not only for the general population but for pregnant patients as well. This trend is of particular concern, because radiation exposure to the fetus may cause deterministic and/or stochastic effects, according to the study authors.
Clinically significant deterministic effects result from radiation doses above a threshold value of 50 mGy to 100 mGy, depending on the sensitivity of the individual, while stochastic risks are a possibility at any dose. Also, gestational age is an important factor, as fetuses are most radiosensitive during the first trimester.
"To date, standard guidelines for CT examinations during pregnancy as well as a systematic overview of associated clinical indications and of radiation doses to the conceptus are largely absent at our university hospital," the researchers wrote.
Therefore, the aim of their study was to perform an internal quality assurance audit to evaluate the number, clinical indication, and operating procedure of CT scans performed on pregnant patients, as well as to estimate radiation doses to the fetus.
 Unknown pregnancy; patient examined within the first 12 weeks for polytrauma.
Unknown pregnancy; patient examined within the first 12 weeks for polytrauma.Study results
The researchers found that CT scans of pregnant patients during the study period consisted of the following types of scans:
- 16 chest CT exams
- 8 abdominopelvic CT exams
- 5 head CT exams
- 2 cervical spine CT exams
The number of CT exams of pregnant patients increased from three to four per year in 2008 to 2011 to 11 per year in 2012, a result that corresponding author Dr. Federica Zanca, also from University Hospitals Leuven, called "surprising" in an email to AuntMinnieEurope.com. In addition, three pregnancies were found by accident on abdominopelvic CT, which Zanca said was also surprising.
Dose to the fetus could be estimated only for 24 of the 31 CT scans and was measured as follows:
| Mean estimated CT radiation dose to fetus | |||
| Exam | Estimated radiation dose (mGy) | ||
| Head CT | 0.01 | ||
| Cervical CT | 0.01 | ||
| Chest CT | 0.03 | ||
| Abdominopelvic CT | 28.7 (range: 6.7-60.5) | ||
The radiation dose for all but the abdominopelvic CT exams were considered negligible, according to the researchers.
"A dose-saving protocol was not routinely used because of the lack of a standardized protocol for scanning pregnant patients with CT at our institution," they wrote. "In some cases, an adapted protocol was selected on the basis of the experience of the technologist and/or radiologist."
How do the results stack up?
The results are largely in line with current literature on clinical indications and typical radiation doses to the fetus during CT exams. In only two of the trauma exams, the estimated doses were much higher than those reported in the literature.
"We should endeavor to reduce the conceptus dose to one as low as reasonably achievable and our hospitals should be aware of the need to implement a radiation protection policy," the researchers added.
Strategies may include tailoring scan parameters to the pregnant patient -- lowering the tube potential and current, increasing the pitch, widening the beam collimation, and reducing the gantry cycle time -- limiting the scan length to the regions of interest, and the use of iterative image reconstruction techniques.
"The ultimate goal is to assess internal guidelines both in terms of protocols to be used when exposing pregnant women and both in terms of the method that can be used to assess dose to the conceptus, in case the radiologist has to communicate this to the patient," Zanca wrote in her email.
The guidelines for her institution are still under development, but the idea is to standardize practices such that they are not operator-dependent, she added.
"In several cases, selection of dose reduction tools like tube current modulation, the use or not of shielding material, or the reduction of scan length was an arbitrary decision of the technologist performing the scan, based on personal experience," she said. "This should be avoided."
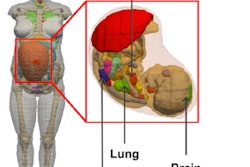
 A patient in her third trimester (29 weeks). Examined for polytrauma.
A patient in her third trimester (29 weeks). Examined for polytrauma.Future research
Zanca and colleagues are currently building a library of voxelized models of pregnant patients of different gestational ages. The models will be used in combination with their framework to estimate dose, which will account for the maternal size and tube current modulation.
The idea is to compare different methods of estimating fetal radiation dose with the scientific literature.
"Base methods to see which one approach is the best to use in clinical practice as the complete simulation sometimes cannot be done," Zanca said. "I guess we will work on the guidelines based on all the elements we have because when a pregnant patient is scanned it's for different reasons therefore it's not a standard procedure."