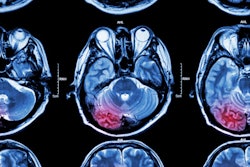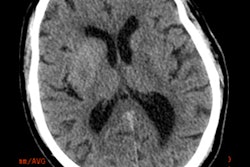
Irish neurologists and radiologists have shown that brain MRI is far more sensitive than brain CT at picking up acute ischemic stroke. In their study presented at last week's U.K. Radiological Congress (UKRC), 26% of MRI scans were positive for stroke in the face of a negative brain CT.
There are no national guidelines as to how quickly MRI should be performed in the case of diagnostic uncertainty following a negative brain CT, noted Dr. Mary-Louise Gargan, senior medical house officer at the neurology at Tallaght Hospital in Dublin. Her group's audit demonstrated that changes can be picked up as early as 24 hours and as late as 12 days, but Gargan and her colleagues recommend caution when ordering a brain MRI scan too quickly because research indicates false negatives are uncommon in the first 24 hours after an ischemic stroke. It is best practice to wait 24 hours before performing brain MRI in the case of a negative brain CT.
"Its (MRI's) role as a highly accurate form of stroke diagnosis has been proven. With the standard stroke protocol, a definite diagnosis of acute ischemia can be made in approximately 10 minutes, making it an invaluable mode of imaging," they stated. "In reality, budget cuts and subsequent lack of resources limit the availability of MRI in Irish hospitals. It is not a 24-hour service, and in some peripheral hospitals, it is not available to all."
The big picture
Stroke is the third most common cause of death and the most common cause of acquired major physical disability in the Republic of Ireland, and imaging plays a critical role in evaluating patients suspected of having an acute stroke, especially prior to initiating treatment, according to Gargan.
They sought to determine the value of brain MRI following the value of brain MRI after negative brain CT in the acute stroke setting, and carried out an audit of the radiology department at Tallaght Hospital, looking at the average length of time between negative brain CT and brain MRI in the acute stroke setting.
All 92 brain MRI examinations performed using the stroke protocol between 1 January 2014 and 30 June 2014 were retrospectively considered for inclusion in the audit. The standard MRI stroke protocol included flair axial, T2 axial, T2* axial, T1 spin sagittal echo, and diffusion-weighted axial (DWI).
The exclusion criteria were that no recent brain CT had been done and the indication for brain MRI was not to diagnose an acute stroke. The inclusion criteria were studies with a clinical syndrome suggestive of stroke, as per the indication on the request form, and studies with a negative initial brain CT followed by a brain MRI within a two-week time frame (time frame varied depending on the availability of MRI).
Imaging exams were reported by several different radiologists, but once they were included in the study, they were reported by two separate consultant radiologists in consensus, to help correlate the accuracy of the reports, Gargan et al explained. A positive brain MRI was taken as a study with an acute lesion reflected by diffusion restriction on DWI.
A total of 73 scans were included in the study. Seven CT scans were excluded on the basis of initial CT findings showing acute ischemia. Two scans were excluded because there was no preceding brain CT. Another 10 were excluded due to the indication for the scan not to evaluate for acute stroke.
Of the scans included in the study, there were 39 men and 34 women patients. The average age was 62.1 (age range 29-86, standard deviation [SD] 14). In total, there were 19 MRI scans positive for acute/subacute infarct, amounting to 26% of the total MRI scans. Of these, 17 were acute and two acute/subacute. The findings were seen as DWI hyperintense lesions with corresponding changes on an ADC map. A total of 13 were left hemispheric and six were right hemispheric. There were 54 negative MRIs performed due to the onset of stroke-like symptoms.
The brain CT scans that were performed pre-MRI were all reported as nil acute. The average time between the CT and MRI scans was 4.7 days (SD 2.603), with a range of 1-12 days (see graph). None of the MRI scans were performed on the same day as the brain CT and therefore none were in the hyperacute phase of stroke.
 Graph depicts the length of time between negative brain CT and brain MRI in Tallaght Hospital.
Graph depicts the length of time between negative brain CT and brain MRI in Tallaght Hospital.CT is the gold standard for the diagnosis of acute stroke, and because most hospitals have 24-hour access to CT, it has remained that way despite evidence showing MRI is more sensitive at picking up acute ischemic changes, even in the early stages of stroke, they continued. DWI appears to be sensitive to an early pathophysiological process in cerebral infarction, the loss of ATP, which causes a sudden shift of water from the extracellular space to the intracellular space. It has been shown to have a sensitivity of 96.6% and specificity of 100%, with a negative predictive value of 90.6%.
Editor's note: This study was also presented as an e-poster at ECR 2015 in Vienna. To read more, click here.