Coronary calcium is a strongly heritable trait, but noncalcified plaque burden is more a factor of lifestyle and environment, according to a new Budapest study of twins presented at the ECR 2015 meeting in Vienna.
"Our research shows that calcified plaque burden has a stronger heritability than total plaque burden, and we believe that total plaque burden's higher influence by the environment is driven mainly by the nonclassified plaque burden," said Dr. Pál Maurovich-Horvat from Semmelweis University in Budapest. "We think that's actually good news because noncalcified plaque burden can be influenced more effectively by lifestyle and therapeutic interventions."
 Dr. Pál Maurovich-Horvat from Semmelweis University in Budapest.
Dr. Pál Maurovich-Horvat from Semmelweis University in Budapest.The comparison of monozygotic (MZ) and dizygotic (DZ) twins' phenotypic similarities can be quantified, but genetic and environmental factors can be determined in a unique way, noted the authors. Their study aimed to determine the magnitude of genetic and environmental impact on coronary calcification and plaque burden.
MZ twin pairs share 100% of their genome, while the DZ twins share 50% of the genome; these percentages are used proportionately to calculate heritability and determine whether characteristics are determined more by genetics or environment, Maurovich-Horvat said. The study determined the correlation values between plaque burden and twin types.
They used a simplified technique known as the Falconer method to analyze the differences. Falconer outputs an H index representing heritability index corresponding with the strength of a genetic determination. Essentially, the scale subtracts observed differences between MZ and DZ twins to determine the degree of hereditability of a trait.
"The larger the difference between the correlation values, the stronger is the genetic determination, and if the difference is small between the monozygotic and dizygotic pairs, then we can conclude that there is a stronger environmental factor in the genetic determinations," Maurovich-Horvat said.
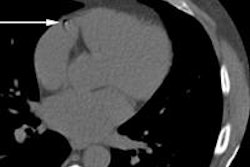
 Coronary CTA of a monozygotic twin pair. The curved multiplanar reconstructions show proximal calcified and partially calcified atherosclerotic plaques (green arrows) of twin A and twin B. All images courtesy of Dr. Pál Maurovich-Horvat.
Coronary CTA of a monozygotic twin pair. The curved multiplanar reconstructions show proximal calcified and partially calcified atherosclerotic plaques (green arrows) of twin A and twin B. All images courtesy of Dr. Pál Maurovich-Horvat.As part of the ongoing Burden of Atherosclerotic Plaques in Twins (BUDAPEST) study, Maurovich-Horvat and his colleagues performed coronary CT angiography in 208 twin subjects, 62 of whom were MZ pairs (mean age 55.7 ± 9.7 years) and 42 of whom were DZ (mean age 58.1 ± 8.7 years). They performed a CT calcium scoring scan as well as coronary CT angiography (CCTA). All twins were asymptomatic with no history of coronary artery disease.
They used a semiautomated Agatston score to determine calcified plaque burden in each individual from native CT scans, and the group also calculated a segment involvement score (SIS), representing the total number of segments with plaque. The segment stenosis score (SSS) was used to represent the sum of all stenoses, including minimal = 1, mild = 2, moderate = 3, and severe = 4. Finally, the SSS index (SSSi) was used to represent the SSS/total segment number, while the SIS index (SISi) represents the SIS/total segment number, the authors wrote in an abstract.
 Coronary artery calcium (CAC) scoring of the same monozygotic twin pair depicted in Figure 1. The proximal LAD plaque CAC score is indicated in green text box for twin A and twin B.
Coronary artery calcium (CAC) scoring of the same monozygotic twin pair depicted in Figure 1. The proximal LAD plaque CAC score is indicated in green text box for twin A and twin B."We normalized these indices based on the total segment number in each [pair of] twins, so the SISi index is basically the segment involvement score divided by the total available segments, and the segment stenosis score is the SSS divided by the total number of segments, so for example if some twin has 15 or 16 segments then we divide the index by 15 or 16," he noted.
Showing a slide of a CT scan of two monozygotic twins' hearts, he explained that the hearts are very similar, but some subtle differences are visible, for example it can be seen that Twin B has a more tortuous coronary vessel.
In summary, the results showed quite similar demographics between the two groups of twins, Maurovich-Horvat said.
| MZ pairs (n = 124) |
DZ pairs (n = 84) |
P value | |
| Age (years) | 55.7 ± 9.7 | 58.1 ± 8.7 | 0.18 |
| BMI (kg/m2) | 28.0 ± 5.0 | 27.7 ± 5.5 | 0.76 |
| Waist circumference (cm) | 98.3 ± 13.9 | 97.5 ± 14.2 | 0.93 |
Both the monozygotic and dizygotic twin types had about a 40% prevalence of calcified plaques, and the stenosis involvement scores also were very similar between twin types at 56% to 58%, respectively.
| Positive subjects % MZ | Median (interquartile range) | Positive subjects % DZ | Median (interquartile range) | P value | |
| Calcium score | 38.7% (n = 48) |
132.3 (27.5 - 387.4) |
40.5% (n = 34) |
107.8 (35.9 - 230.3) |
0.88 |
| SSSi | 55.6% (n = 69) |
0.3 (0.1 - 0.5) |
58.3% (n = 49) |
0.2 (0.1 - 0.4) |
0.97 |
"You can appreciate that there was about 16% to 17% of noncalcified plaque burden only, because SSSi and SISi include noncalcified plaques," Maurovich-Horvat explained.
As for the Falconer-scale based heritability of coronary artery plaque however, MZ versus DZ showed important differences in calcified plaque burden depending on twin type, 0.71 versus 0.21, with monozygotic twins tending to have very similar calcified plaque burdens, while total plaque burdens -- mostly representing noncalcified plaques -- were not correlated with twin type.
| rDZ | rMZ | h2 (Falconer-based heritability index) | |
| Calcium score | 0.71 | 0.21 | 1.015 |
| SSSi | 0.54 | 0.22 | 0.632 |
| SISi | 0.39 | 0.15 | 0.466 |
The results showed that calcified plaque burden has stronger heritability than total plaque burden, Maurovich-Horvat said. And because the influence of the environment in total plaque burden is driven mainly by noncalcified plaque burden, the good news is that lifestyle changes and medication can potentially change the outcomes of twins with noncalcified plaques. The process does need some improving, and more twin pairs need to be studied, however.
"Next we are planning a fully automated plaque quantification in order to improve our heritability estimations," he said. In response to a question from the moderator, Maurovich-Horvat said that similarities in myocardial bridges are quite stark among MZ twins, with results to be reported next year.