In patients with stable angina and suspected coronary disease, a "tiered" approach to CT imaging finds -- so far at least -- that calcium scoring is all many patients need. That's right, for most patients there's simply no need to start with the big imaging guns, researchers in Rotterdam report.
What's a tiered approach to patients with suspected coronary disease? Ironically, it's a plan to minimize CT use while depending on the modality completely, Dr. Koen Nieman noted in a presentation at last month's International Symposium on Multidetector-Row CT.
"We've realized that the prevalence of coronary artery disease in a standard outpatient clinic is actually very low, and does not coincide with what we've seen in the population," he said. "The prevalence is not usually more than 10% or 20%. So what we do with these patients is we have a calcium scan first, and 30% to 40% of patients we can rule out. We will not tell them that they have no atherosclerosis, but we will tell them that the risk of having coronary artery disease is very low -- and if they keep having symptoms they are welcome to come back."
The approach remains controversial, of course, but the Rotterdam team is confident it's on the right track. "We take a comprehensive approach to coronary artery disease using different tools we have with CT -- and we provoke some new ideas that some may agree with," said Nieman, who is an associate professor and director of cardiovascular imaging research at Erasmus University.
 The tiered approach. All images courtesy of Dr. Koen Nieman.
The tiered approach. All images courtesy of Dr. Koen Nieman.CT has been around to image the coronary arteries for about a quarter century, and while it's been a good thing, it has its limitations. CT is best for excluding coronary artery disease in patients with a low-to-intermediate probability of disease, and that's a job it does very well, he said.
"But sometimes it's difficult to tell in positive findings whether that's actually true in an angiographic sense and particularly in a hemodynamic sense," he said. And despite CT's prowess for ruling out disease, "there are some situations where you may wonder whether CT is actually the right technology," for example, "in patients with heavy calcifications or arrhythmia where CT turns out to be nondiagnostic and you wonder if perhaps CT wasn't particularly suited in those situations."
If CTA shows moderate obstructive disease, for instance, one might wonder whether the lesion is really hemodynamically significant "and you still don't know what the next step will be," he said. "And then in our patient with perfectly normal arteries where we can rule out coronary artery disease and you wonder whether it was really necessary to perform a CT angiogram."
Calcium score sufficient to rule out CAD?
At Erasmus they're starting with a coronary artery calcium score to rule out most obstructive disease. The test isn't used for prognostic purposes, Niemen said, "but for the simple fact that it's quite rare to have severe diagnostically relevant coronary artery disease in the absence of calcium. Some studies, mostly in catheterization populations, do show a substantial portion of patients with 50% obstructive disease, and these patients are getting revascularized," he said. "But these are not the patients we see in outpatient clinics."
In his group's 2009 study in the American Journal of Cardiology (1 Dec 2009, Vol. 104:11, pp. 1499-1504) "we found that in patients that do not have calcifications the number with more than 50% disease is actually less than 2%," he said. In another Dutch study, by Mouden et al (Radiology, October 2013, Vol. 269:1, pp. 77-83), 12% of the patients had abnormal myocardial perfusion imaging "but CT angiography didn't show obstructive disease in any of them, not even a few," Neiman said.
Finally, results of the Coronary CT Angiography for Clinical Outcomes (CONFIRM) trial (Shaw et al, Journal of the American College of Cardiology, 13 November 2012, Vol. 60:20, pp. 2103-2114) deliver essentially the same conclusion in terms of prognostic outcomes. In 3.7% of patients with more than 50% obstructive disease at CCTA, revascularization was actually needed in less than 1%.
"That makes you wonder whether [CCTA] is really necessary for this relatively benign disease," he said. "Let's be honest about it: Most patients with stable angina will not drop dead immediately... The yield of CCTA is actually quite low."
The U.K. guidelines for chest pain of recent onset (NICE 2009) support the conclusion that in a patient with a low pretest probability of coronary artery disease "you can get away with a calcium test," he said. "If it's negative you really should consider other causes of disease." Similarly, American guidelines from the American College of Cardiology and the American Heart Association suggest the possibility of a calcium score in patients with a low probability of coronary artery disease, although it's not a strong recommendation.
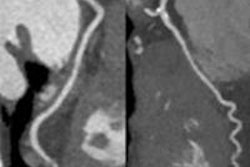
CTA in patients with high calcium scores
In contrast to patients with a low calcium score, those with high scores have a very high likelihood of finding obstructive disease -- in fact, it's hard to exclude obstructive disease when calcium scores are very high, Nieman said.
"But it doesn't mean [CCTA] is a nonuseful test," he noted. "We often find patients with single-vessel disease that we detect at CTA that we don't send to the cath lab. We know that patients with single-vessel disease and two-vessel disease in small vessels do not have any prognostic benefit from immediate revascularization, so unless the symptoms cannot be reduced using medication there's no reason to put in a stent."
The question of the functional significance of a stenosis remains valid, however, and it can be addressed by a number of tests, for example cardiac perfusion, he said. Several groups have shown that if you do CTA and use functional endpoint as the diagnostic endpoint then CTA has very high sensitivity but relatively poor specificity, he said. Adding myocardial blood flow CT perfusion adds substantially to the exam, increasing positive predictive value compared with CTA. Negative predictive value dips a little but still remains high.
The group's calcium-centric protocol is pretty straightforward. Start with calcium scoring to rule out 30% to 40% of the patients with low scores and a very low probability of disease. When calcium is positive in a patient with a low pretest probability of disease, CTA does a good job of ruling out relevant disease. Patients with one- or even two-vessel disease can start an optimum medical therapy regimen before the doctors consider doing anything else. If myocardial ischemia is a concern -- it is in perhaps one out of six or eight patients -- then immediate myocardial perfusion imaging can give the answers, and at this point patients with functionally significant disease will be cathed, he said.
 The Crescent trial.
The Crescent trial.To validate their ideas, Neiman and his colleagues have started their Crescent Pilot study, which will follow some 250 patients with suspected coronary disease prospectively in three centers using the tiered algorithm, Nieman said. They will be followed up for death, myocardial infarction, complaints, quality of life, and costs. "We want to repeat it in a larger population if our results turn out to be promising," he said.