When patients arrive in an accident and emergency (A&E) department showing symptoms of a myocardial infarction, a catheter-based examination may be inconclusive, but nine times out of 10 MRI will lead to the correct diagnosis, according to a study presented at last week's 95th congress of the German Society of Radiology (DRK).
 At the DRK, Dr. Tilman Emrich presented results from a study demonstrating that cardiac MRI enables high diagnostic confidence in cases of nondescript chest pain.
At the DRK, Dr. Tilman Emrich presented results from a study demonstrating that cardiac MRI enables high diagnostic confidence in cases of nondescript chest pain.
Consider this case, which is anything but uncommon: A patient admitted to the A&E unit suffers from nondescript chest pain, hinting at a myocardial infarction. Lab results may support this suspected diagnosis, showing elevated levels of the cardiac enzyme troponin. The cardiologist will carry out a catheterization, but will not find an acute lesion in any of the three coronary arteries or their main branches.
"A multitude of studies have shown that many patients with equivocal catheterization findings actually do suffer from a cardiac disease. In cases where echocardiography -- incapable of showing scars or edemas -- does not produce any clear results either, patients may be sent home again without any diagnosis," said Dr. Tilman Emrich, from the Department of Diagnostic Radiology at Mainz University Hospital, adding that CT does not provide any additional information, but in such cases, cardiac MRI can help.
The major benefit of MRI is that it visualizes both the anatomy and the function of the heart in detail, and this makes it possible to detect conditions of the muscle as well as impaired wall motion and issues regarding oxygen supply or the pumping function. Emrich's team used cardiac MRI to examine 125 patients presenting with chest pain, elevated levels of troponin, and uncertain catheterization results. A diagnosis was established based on results from the MRI examination. A diagnosis based on the consensus of experts, including radiologists and integrating the subsequent clinical progression, served as a reference.
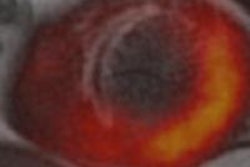
 Acute myocardial infarction. General MRI features include regional wall motion abnormality, myocardial edema corresponding to regional wall motion abnormality, subendocardial to transmural late-enhancement (depending on infarct severity), and embolic infarction in side wall of left ventricle. All images courtesy of Dr. Tilman Emrich.
Acute myocardial infarction. General MRI features include regional wall motion abnormality, myocardial edema corresponding to regional wall motion abnormality, subendocardial to transmural late-enhancement (depending on infarct severity), and embolic infarction in side wall of left ventricle. All images courtesy of Dr. Tilman Emrich."Our study demonstrated that, even if catheterization results are equivocal, many conditions of the heart muscle were prevalent in these patients," Emrich emphasized.
For 90% of these cases, cardiac MRI yielded the correct result, as was shown by a comparison with the reference diagnosis. Conditions associated with chest pain and elevated troponin levels include myocarditis, dilatative cardiomyopathy, Takotsubo cardiomyopathy, and hypertensive heart disease. In some cases, a myocardial infarction was shown that had not been detected by catheterization.
 Takotsubo cardiomyopathy, also known as transient apical ballooning syndrome or stress cardiomyopathy. General MRI features include regional ventricular ballooning (apical, as in this case, and sometimes midventricular or basal), reduction of left ventricular ejection fraction, myocardial edema corresponding to regional wall motion abnormality (not shown), and absence of significant fibrosis/necrosis on late enhancement imaging (not shown).
Takotsubo cardiomyopathy, also known as transient apical ballooning syndrome or stress cardiomyopathy. General MRI features include regional ventricular ballooning (apical, as in this case, and sometimes midventricular or basal), reduction of left ventricular ejection fraction, myocardial edema corresponding to regional wall motion abnormality (not shown), and absence of significant fibrosis/necrosis on late enhancement imaging (not shown)."Cardiac MRI permits high diagnostic confidence," Emrich summarized. "As a result of our study, we recommend that for all cases of nondescript chest pain with accompanying lab results hinting towards a myocardial infarction and with inconspicuous catheterization, cardiac MRI should be used. Patients will profit from a correct diagnosis and suitable subsequent therapy."
 Hypertensive heart disease. General MRI features include concentric hypertrophy of the left ventricular (LV) myocardium, end-diastolic thickness of interventricular septum >13 mm, impaired systolic LV function, scattered zones of late enhancement, and sometimes (as in this case) diffuse edema pattern.
Hypertensive heart disease. General MRI features include concentric hypertrophy of the left ventricular (LV) myocardium, end-diastolic thickness of interventricular septum >13 mm, impaired systolic LV function, scattered zones of late enhancement, and sometimes (as in this case) diffuse edema pattern.As for the prognosis, the primary endpoints are MACE (major adverse cardiac events: death, stroke, heart failure), recurrent hospitalization, and the de novo interventional procedure, he concluded.