CT is not significantly different from ultrasound in identifying ovarian torsion, according to an article in press from the European Journal of Radiology. The study results suggest when CT demonstrates ovarian torsion findings, another imaging exam (such as ultrasound) is unlikely to improve preoperative diagnostic yield.
Ovarian torsion is a rare but serious cause of acute abdominal and pelvic pain in women. Associated clinical signs and symptoms of torsion are nonspecific, and overlap an extensive range of gynecologic, genitourinary, and gastrointestinal etiologies of pain. The workup for women presenting to the emergency department (ED) with acute lower abdominal or pelvic pain often involves diagnostic imaging with either ultrasound or CT (EJR, 8 January 2014).
Pelvic ultrasound has been considered the modality of choice due to its ability to directly evaluate ovarian anatomy and perfusion, as well as its low cost and lack of radiation. However, ultrasound can be limited by interoperator variability, nighttime availability in smaller community hospitals, and utility for diagnosing nongynecologic etiologies of pain. Also, given that the signs and symptoms of torsion are nonspecific, CT is often performed, particularly when other etiologies for pain are suspected.
In light of ultrasound's imperfections and CT's potential to exclude torsion, Dr. David W. Swenson, from the Alpert Medical School of Brown University at Rhode Island Hospital in Providence in the U.S., and colleagues compared the two modalities in women presenting to the ED with acute lower abdominal or pelvic pain related to ovarian torsion.
Their retrospective study included 20 cases of ovarian torsion and 20 control patients, all of whom had both ultrasound and CT performed in the emergency department. CT exams were obtained on one of several multidetector-row scanners: GE Healthcare's BrightSpeed Elite 16, Lightspeed VCT 64, or Siemens Healthcare's Sensation 16. Ultrasound exams were obtained on one of two high-resolution ultrasound units, Philips Healthcare's IU22 or GE's Logiq 9.
Two radiologists who were blinded to clinical data interpreted all studies as demonstrating an abnormal ovary or not, and suggestive of torsion or not.
| CT vs. ultrasound for ovarian torsion | ||||||
| Abnormal ovary on pelvic ultrasound | Abnormal ovary on CT | Pelvic ultrasound for torsion sensitivity | Pelvic ultrasound for torsion specificity | CT for torsion sensitivity | CT for torsion specificity | |
| Reader 1 | 90% | 100% | 80% | 95% | 100% | 85% |
| Reader 2 | 100% | 100% | 80% | 85% | 90% | 90% |
"In this small series, these results contradict the common thinking that pelvic US [ultrasound] is superior to CT for evaluating ovaries in the acute setting," they wrote.
However, the researchers' retrospective review of pelvic ultrasound studies is inherently limited by the inability of the interpreting radiologists to directly perform real-time scanning.
Additionally, the control population was matched for age and symptoms, but the incidence of adnexal pathology in the controls was low, including 10 of 20 (50%) described as having any adnexal abnormality on either ultrasound or CT, and only two of 20 (10%) with reported surgical intervention to provide definitive pathology.
"Given that the most common imaging finding in cases of torsion is an abnormally enlarged ovary, further study with a control group consisting of patients with an enlarged ovary that is surgically confirmed to be nontorsed would be interesting," they added. "Such a control population would be expected to decrease the specificity of both US and CT imaging for torsion, although sensitivity would likely remain high, allowing torsion to be excluded in the acute setting."
Also, given the relative rarity of ovarian torsion, a control group with larger numbers of controls would more closely mimic actual clinical practice.
A CT exam demonstrating bilateral normal ovaries may effectively exclude torsion as an etiology for acute pain, but the presence of an abnormal ovary on CT must be considered suspicious for torsion in the acute setting.
"The sensitivity and specificity of CT are not shown to be significantly different from that of US in diagnosing ovarian torsion," the authors concluded. "Radiologist familiarity with the findings of ovarian torsion on CT may expedite accurate diagnosis and urgent surgical intervention."
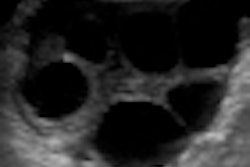
CT signs of torsion include ovarian stromal heterogeneity or edema, numerous small peripheral follicles, inflammatory stranding of the paraovarian fat, a twisted vascular pedicle, pelvic free fluid, and deviation of the uterus toward the side of torsion.
Additionally, appreciation of CT's high sensitivity for identifying an abnormal ovary in the setting of torsion may allow clinicians to avoid unnecessary additional imaging with pelvic ultrasound when a CT demonstrates normal bilateral ovaries.
"This is increasingly relevant as CT is often the first imaging modality performed for acute undifferentiated lower abdominal or pelvic pain in women," they wrote.