Gynecological emergencies don't just happen during pregnancy. Researchers from a top London hospital have compiled an overview of the imaging appearances of emergencies in nonpregnant patients, and they found MRI is particularly helpful in identifying the site of origin of large pelvic masses such as torsion.
Acute abdominal pain related to the gynecological tract is a common occurrence. One of the challenges physicians face is the wide range of differential diagnoses that must be considered when assessing the problem, according to Dr. Óran Roche, a radiologist from St. Bartholomew's Hospital in London, and colleagues (Insights into Imaging, 18 April 2012).
 |
| Endometrioma: Patient presented to the emergency department with lower abdominal pain that became worse during menstruation. Subsequent transvaginal ultrasound demonstrated heterogeneous echotexture. Hypoechoic regions are a result of organizing hemorrhagic debris within hyperechoic septations and wall foci. Anechoic cysts may occur, but they are rare. All images courtesy of Dr. Óran Roche. |
 |
"Often it can be difficult to distinguish gynecological from gastrointestinal emergencies," the authors wrote. "In conjunction with clinical findings, various imaging modalities play an important role in diagnosing the cause of pain."
 |
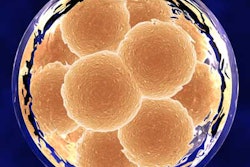
| Although not a typical acute gynecological presentation, this patient presented with abdominal distension, nausea, and vomiting. This transvaginal ultrasound demonstrated symmetric enlargement of the left ovary; however, both ovaries were similar in appearance (often they can be more than 12 cm in size) with multiple cysts of varying sizes. Ovarian hyperstimulation syndrome can also be present with ascites and pleural effusion. Pericardial effusion (due to capillary leak) can also be present. |
Physicians usually use ultrasound when patients present with pain originating in the gynecological tract because ultrasound is highly sensitive, fast, and easy to access. CT is rarely used as an initial diagnostic tool because of the risks associated with irradiating the pelvis.
"However, it may be difficult to localize the site of origin of the symptoms to the gynecological tract due to the significant overlap in symptoms and signs with gastrointestinal pathologies, and CT may be selected as the first imaging modality," they noted. MRI isn't usually used in the acute setting, they added, but it may be beneficial when characterizing abnormalities that remain indeterminate following ultrasound or CT.
Ultrasound, on the other hand, can identify hemorrhagic follicular cysts, ovarian cyst rupture, endometriotic cysts, pyosalpinx, and adnexal torsion. However, adnexal torsion cannot be safely excluded using ultrasound alone.
"In cases of suspected acute gynecological disease, the findings on imaging must be interpreted in association with the clinical presentation," the authors stated. The pregnancy status of the patient must also be established to exclude ectopic pregnancy and to avoid using imaging modalities that could harm the fetus.
 |
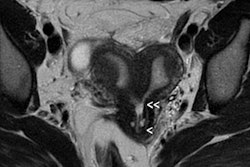
| Pyosalpinx: Patient presented with lower abdominal pain and increased inflammatory markers. Transvaginal ultrasound demonstrated dilated serpentine structures with internal echogenic debris representing infective pus within the fallopian tubes. |
 |
Here is what to look for regarding certain gynecological presentations, according to the authors:
- Hemorrhagic ovarian cysts: These display internal reticular patterns on ultrasound with high-attenuation contents on noncontrast CT, an enhancing cystic wall, and contrast-enhanced blood in the pelvis on delayed phases in cases of cyst rupture.
- Endometriotic cysts: These have a ground-glass appearance on ultrasound and characteristic high signal intensity on T1- and shading on T2-weighted MRI.
- Adnexal torsion: Doppler can demonstrate whirlpool or corkscrew signs of a twisted vascular pedicle. Contrast-enhanced CT and MRI may show reduced enhancement in the twisted ovarian mass, another diagnostic feature of torsion. It should also be noted that when torsion is suspected clinically but diagnostic imaging features are not demonstrated, imaging cannot be relied upon to confirm the diagnosis.
- Fibroid degeneration: MRI is the most effective modality. Red degeneration demonstrates high signal intensity centrally on T1-weighted images due to acute blood and a low signal periphery on T2 due to hemosiderin deposition. Submucosal pedunculated leiomyomas can demonstrate a "broccoli sign" with heterogeneous signal due to the characteristic stalk linking the herniating fibroid with the endometrial cavity.
- Complications of pelvic inflammatory disease: These may be seen on ultrasound as dilated fallopian tubes with internal echogenic debris being a typical feature of pyosalpinx. CT and MRI may demonstrate typically bilateral dilated fallopian tubes and inflammatory changes in the adjacent fat planes.
"Overlap in the presenting features of acute gynecologic disease and gastrointestinal disease remains a significant challenge in the emergency department and imaging plays an important diagnostic role," the authors concluded.