Computer-aided diagnosis (CADx) shows potential as a tool to aid radiologists in the challenging task of finding cancer originating from the prostate's central gland, according to Dutch research presented at the 2012 RSNA meeting in Chicago.
In a study of the institution's CADx system on 101 patients, researchers from Radboud University Nijmegen Medical Center's Diagnostic Image Analysis Group found the software yielded similar performance to that achieved by radiologists in a prior study in the literature.
"A CAD system based on texture and relaxation features can achieve a prostate cancer diagnosis performance approaching that of radiologists using T2-weighted MRI," Geert Litjens said. "We hope that this will eventually lead to a complete system [that] will help improve the diagnostic accuracy of the radiologists."
Litjens presented the team's work during a scientific session at the conference.
Seventy percent of prostate cancers originate in the peripheral zone of the prostate, while 30% come from the central gland; as a result, most clinical and CAD research in prostate MRI focus on the peripheral zone. However, central gland lesions are difficult to diagnose on MRI, Litjen said.
In men with persistently high prostate-specific antigen blood test results and one or more negative transrectal ultrasound biopsies, multiparametric MRI is performed with T2-weighted, diffusion-weighted, and dynamic contrast-enhanced imaging. In these patients, approximately 50% of cancers are found in the peripheral zone and approximately 50% are found in the central gland, he said.
"This is most likely caused by the fact that due to the anatomy of the prostate, cancer in the central gland is most difficult to biopsy," Litjens told AuntMinnieEurope.com. "Due to the distributions of cancer origin found in [transrectal ultrasound or TRUS], a lot of studies have focused on the detection of prostate cancer in the peripheral zone, neglecting the 30% of cancers -- and even more in MRI after initial negative TRUS biopsy -- originating in the central gland."
Because the recently published Prostate Imaging Reporting and Data System (PI-RADS) described texture characteristics as the most important feature in detecting cancer in the central gland, the researchers decided to develop a CADx system to differentiate between normal/benign and malignant areas using texture and relaxation features, Litjens said. Relaxation features (T2 maps) are needed due the lack of standardization in MR signal intensity.
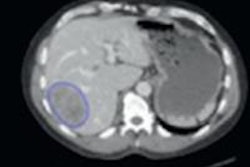
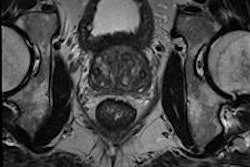
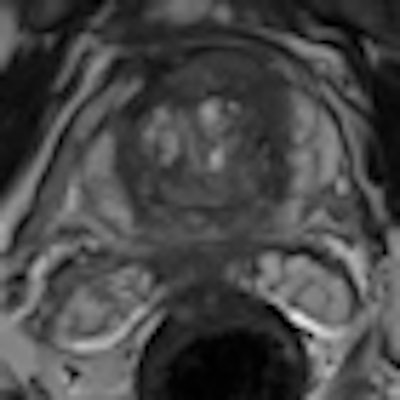
 CADx software shows promise for improving detection of prostate cancer lesions originating in the central gland. All images courtesy of Geert Litjens.
CADx software shows promise for improving detection of prostate cancer lesions originating in the central gland. All images courtesy of Geert Litjens.Making use of these texture and relaxation features, the system performs linear discriminant analysis including sequential forward floating feature selection (SFSS). It then constructs a feature vector for each voxel in an annotated region and classifies each feature vector, yielding a cancer likelihood per voxel, Litjens said. The region summary statistic is the 75th percentile of all voxel likelihoods.
The researchers then evaluated their system on 101 patients, 36 of whom had benign disease and 65 of whom had MR-guided biopsy-proven prostate cancer. Each region was contoured using a countering tool.
 Receiver operating characteristic (ROC) curve for CADx in central gland lesions.
Receiver operating characteristic (ROC) curve for CADx in central gland lesions."Our results show that an area under the [receiver operator characteristics (ROC)] curve of 0.76 can be achieved using our method, which is similar to the performance of radiologists reported in literature when they only have T2-weighted images available," Litjens said.
Litjens noted there was no direct comparison to radiologist performance in their study. Also, more MRI parameters such as diffusion-weighted imaging (DWI) and dynamic contrast enhancement (DCE) can further help improve the system, he said.