Emerging 3D turbo spin-echo (TSE) sequences with isotropic resolution are increasingly valuable for assessing the knee joint at 3 tesla, but they cannot be used as a single sequence, and MR protocols at 3 tesla must include both 2D and 3D TSE sequences, Belgian researchers have found.
3D sequences are now commercially available on many MR vendor platforms, and they include 3D fast spin-echo Cube (GE Healthcare), 3D Fourier Transform (FT, Philips Healthcare), and sampling perfection with application optimized contrasts using different flip-angle evolutions (SPACE, Siemens Healthcare).
"The advantage of the new 3D TSE acquisitions is their capability of mimicking the contrast properties of conventional 2D TSE proton-density weighted acquisitions. In addition, high-quality multiplanar reformatted images may be created in any orientation from the volumetric source data," noted Dr. Pieter Van Dyck, a senior staff member of the division of skeletal radiology at University Hospital Antwerp.


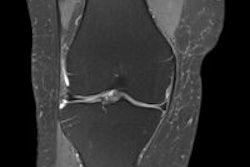
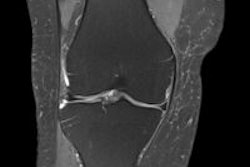
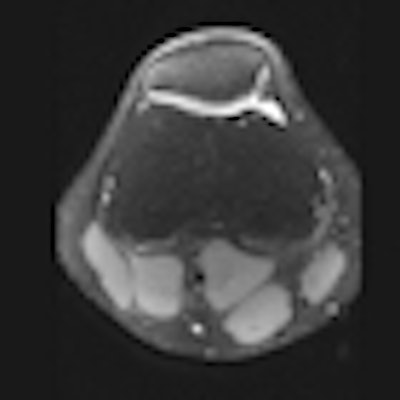
 3D SPACE sequence performed at 3 tesla in a 21-year-old man. All scans are 1-mm multiplanar reformatted images in the sagittal (left), axial (middle), and coronal (right) plane. The patient had no abnormalities at arthroscopy. This case illustrates that all relevant structures (menisci, ligaments, and cartilage) can be visualized well using this sequence with good contrast-to-noise ratio between cartilage/meniscus and synovial fluid. All images courtesy of Dr. Pieter Van Dyck.
3D SPACE sequence performed at 3 tesla in a 21-year-old man. All scans are 1-mm multiplanar reformatted images in the sagittal (left), axial (middle), and coronal (right) plane. The patient had no abnormalities at arthroscopy. This case illustrates that all relevant structures (menisci, ligaments, and cartilage) can be visualized well using this sequence with good contrast-to-noise ratio between cartilage/meniscus and synovial fluid. All images courtesy of Dr. Pieter Van Dyck.Because uncertainty remains as to whether a single 3D TSE acquisition can replace the multiple conventional 2D acquisitions, studies are needed to determine the diagnostic usefulness of 3D TSE in future knee MR protocols at 3 tesla, Van Dyck and colleagues wrote in an article published online on 26 October by Insights into Imaging. The purpose of their retrospective study was to assess the diagnostic performance of the 3D TSE SPACE sequence, as compared with routine 2D TSE sequences, for evaluating the menisci, anterior cruciate ligament (ACL), and cartilage of the knee joint in symptomatic patients at 3 tesla.
Between January and July 2011, they added isotropic 3D SPACE to a 2D knee protocol at 3 tesla. The study included 40 patients: 25 men and 15 women with an average age of 43 and a range of 18-78 years. They had no prior history of knee surgery and had undergone a 3-tesla MR of the knee, consisting of 2D TSE sequences and the 3D SPACE sequence. The patients had subsequent knee arthroscopy. The mean time interval between MR and arthroscopy was 46 days (range 3-112 days).
Three readers independently assessed MR images for meniscus, ACL, and cartilage lesions. The first two readers evaluated 3D and 2D data at separate sittings, and the third reader interpreted the complete examinations, including 3D and 2D sequences.
All MR knee examinations were performed with a single 3-tesla system (Trio TIM Magnetom; Siemens Healthcare) and an eight-channel phased-array knee coil with the same imaging protocol. The imaging protocol consisted of standard 2D TSE acquisitions and a SPACE 3D TSE acquisition. The 2D protocol consisted of a coronal fat-suppressed (FS) TSE intermediate-weighted (IM-w) acquisition, an axial FS TSE IM-w acquisition, and a coronal SE T1-weighted acquisition, according to the authors.
The 3D protocol consisted of a single 3D TSE acquisition in the sagittal plane with the SPACE sequence. The SPACE isotropic source data were postprocessed on a workstation (Leonardo, Siemens Healthcare) to create sagittal, coronal, and axial multiplanar reformatted (MPR) images with 1-mm slice thickness. Readers were free to use volumetric data to create MPRs in any orientation and slice thickness, they stated.
Accuracies were calculated using arthroscopy as reference standard. McNemar's test (p < 0.05) was used to compare 3D and 2D techniques. The highest diagnostic yield was obtained by the third reader (accuracies ≥ 88%). For the medial meniscus, readers performed better with the 2D technique than with 3D SPACE (accuracies 85%-88% versus 78%-80%, respectively) (p > 0.05). For the lateral meniscus and ACL, 3D and 2D techniques had similar performance (accuracies ≥ 93%). For cartilage lesions, 3D SPACE had significantly lower specificity than the 2D protocol for one reader.
An important limitation of the study was the relatively small patient population. Chance fluctuations causing differences in MR accuracy can occur even with sample sizes as large as 100, but a study including more than 100 patients would not have been possible in a busy clinical practice, noted Van Dyck and colleagues. Also, they did not obtain 2D sagittal images because of time constraints, although accurate assessment of the knee joint could be made using coronal and axial 2D sequences, as indicated by the high accuracy rates obtained by reader one and two for all lesions, they wrote.
The researchers admit that the arthroscopy findings could have been biased by the availability of the MR reports introducing surgical bias and limiting the reference standard. Also, selection bias was introduced, as the study group consisted of only a proportion of all patients undergoing MR of the knee at their hospital.
Overall, the study shows the 3D SPACE sequence needs further optimization regarding image quality and further acceleration of acquisition for improving time efficiency and patient comfort, they concluded. Until this goal is achieved, 3D SPACE cannot be used as a single sequence in the MR evaluation of the knee at 3 tesla.