Radiologists have a hard-wired tendency to follow their intuition, but they need to override this by awakening the part of their brain that rigorously questions the image before their eyes, a senior radiologist told delegates at last week's U.K. Royal College of Radiologists annual meeting in London.
The brain has two systems that may be used to interpret an image: "System one" is automatic and intuitive, and "system two" involves logic and reasoning, according to Dr. Adoni Toms, consultant radiologist at Norfolk and Norwich University Hospital in Norwich, U.K.
"It's important for radiologists to be aware of how the two systems of the brain work together," he said in a postmeeting interview with AuntMinnieEurope.com. "When we get a slightly uncomfortable feeling about a film, we need to be aware that this is system two nagging us, and we need to wake up and check it out. Don't let system one fool you into letting it go, even if you are a senior expert."
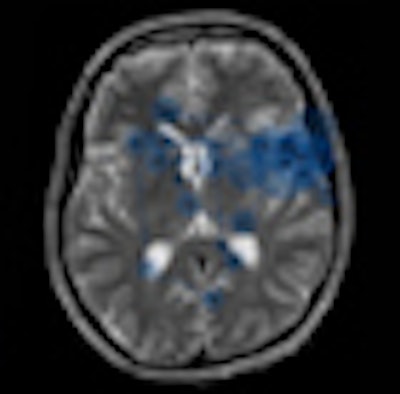
 This eye-tracking overlay was designed to avoid visual and cognitive errors, and was developed at the University of Loughborough. It was originally presented at the SPIE 2010 meeting. Image courtesy of Lindsey Cooper, Alastair Gale, PhD, and Dr. Adoni Toms.
This eye-tracking overlay was designed to avoid visual and cognitive errors, and was developed at the University of Loughborough. It was originally presented at the SPIE 2010 meeting. Image courtesy of Lindsey Cooper, Alastair Gale, PhD, and Dr. Adoni Toms.It comes as no surprise that the system one of a senior consultant is far more honed to spot an abnormality than that of a more junior colleague. Reporting on previous work with psychologists Alastair Gale, PhD, a professor, and Lindsey Cooper at Loughborough University in the U.K., Toms explained findings on how the brain's image perception systems function by tracking eye movement across images in trainees from year one to year five-plus. Clear differences in spotting abnormalities were found. Senior consultants (five or more years) spotted an abnormality in less than 200 msec and then looked for secondary features around the initial abnormality.
"Trainees approached it more randomly, and looked for patterns of symmetry and asymmetry. Novices looked for pretty patterns," he reported.
These subconscious differences between radiologists result from experience and the number of images seen over time. If a radiologist doesn't get the numbers in, then they won't get the hard wiring, noted Toms, adding that the eye movement findings in senior consultants have to be subconscious.
"It cannot be a systematic working through of the image. It is system one, which only works with a brain that has seen thousands of these images," he said. "This intuition only comes with experience in a particular field or task."
However, Toms added that to an extent, all radiologists -- senior or not -- instantly recognize certain information. He invited the audience to read a brain CT image for 200 msec that he flashed on the screen. Everyone easily recognized the abnormalities. "This is recognition using subconscious thought processing: system one," he explained.
Toms then asked how many of the delegates had finished a two-hour reporting session and thought, "I can't remember any of the cases I looked at." With amusement, most of the audience could relate to this experience. "This shows system one at work, which is very efficient and useful for many experiences in life, but not necessarily radiology," he added.
He then showed how system two worked by challenging the attendees with a difficult multiplication that would require most people to use pen and paper or at least more brain power to figure out the answer. "This is system two. You need to concentrate hard," he said.
It is the weaknesses in the way the two systems of brain processing work together that lead to mistakes in interpretation of images. Toms demonstrated this by showing two horizontal parallel lines, one with inward-pointing arrows at the ends, and the other with outward pointing arrows, known as the Müller-Lyer illusion from 1889.
 The Müller-Lyer illusion from 1889.
The Müller-Lyer illusion from 1889.
"We automatically think one line is longer than the other, but another part of our brain says, 'No, I know they are both the same because I've seen this before.' Still, our system one says, 'The bottom line is shorter!' This is system one overpowering the logic of system two, showing system one is the dominant thought process," he explained. "System one provides an answer; system two wakes up slightly but then thinks, 'I can't be bothered. Let's go with system one.' System two is lazy; it requires too much hard work. The same thing happens in radiology. A difficult case goes up and we think, 'That's not quite right, but it's lunch time. Let it go.' "
In fact, a study that investigated the number of missed pulmonary nodules on lung images showed that all of the missed nodules had actually been held in the gaze of the observers for at least 200 msec. When the radiologists were later asked if they had seen the missed nodule, they said they had not. "System one has made the decision and let it go. They are completely unconscious that they've made that decision," Toms said. "We need to activate system two."
System two also tires easily. Toms explained that while using system two you do not necessarily require a break but a change. "Repeating a task over an hour allows a pattern or rhythm to get going, but activities need to be blocked into chunks to avoid fatigue," he said.
Toms added that various experiments had also shown that words, images, and other forms of priming can influence how the brain interprets information. "If there is an area of high misses, there are ways of priming radiologists to try and spot these before reporting the images -- for example, major misses such as masses behind the heart, or apical lung cancers. Priming might involve images or a movie," he said. "Advertisers prime us all the time -- it's very powerful. It might help difficult diagnoses."
Clinical history provides a classic example of priming, and there is a strong argument to avoid looking at the clinical history before seeing the images because it will prime for one particular finding. Placing false cases into each reporting session might prime radiologists to look for particular abnormalities, Toms added.
Illustrating another aspect of how our brains process information, Toms used research on handwriting to show that if it was relatively illegible, we would not bother to read it. If it was too clear, then we would make a mistake reading it. But if it was moderately legible, then the brain needed to concentrate harder and fewer mistakes were made. "It's paradoxical but if the brain has to work harder, then system two is activated, so some cognitive strain is good," he said.
Returning once more to the benefits of eye tracking radiologists while viewing images, Toms argued that it might be valuable to test trainees with eye-tracking programs in addition to the lengthy training they already receive. "Even if the trainee is approved as having a consultant-level ability to read images, it doesn't mean they have seen enough cases to be hard-wired," he said. "An eye-tracking examination would tell you if the trainee has a consultant pattern of abnormality recognition, and we would know they are now hard-wired for this. Just counting the number of cases reported doesn't necessarily mean they've got it."
Toms' colleague Gale has specialized in radiological errors for more than 40 years, and has extensive experience in eye tracking of radiologists. His group also carries out research into homeland security and other areas where people make visual and cognitive errors. In breast screening, the team runs a national self-assessment scheme, which has run now for more than 25 years and helps radiologists identify early signs of breast cancer. The group is going to make this scheme available internationally later this year.
|
Key points/take home messages from Dr. Toms' RCR presentation
|
















