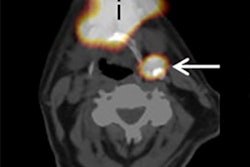
Using SPECT/CT scans to guide the excision of sentinel lymph nodes in melanoma patients produced both a greater rate of metastasis detection and higher disease-free survival rates, according to a German study published in the 12 September issue of the Journal of the American Medical Association.
Researchers from the University of Duisburg-Essen concluded that a preoperative 3D SPECT/CT scan could also help overcome the high false-negative rate of sentinel lymph node excision by providing additional anatomical information to the surgeon.
According to the World Health Organization, the incidence of melanoma is increasing faster than any other cancer in the world; currently, it's the third most common cancer in Australia and the fifth most common cancer in the U.S. The American Cancer Society estimated that approximately 70,230 new melanomas were diagnosed in the U.S. last year, resulting in approximately 8,790 deaths (JAMA, 12 September 2012, Vol. 308:10).
Lead study author Dr. Ingo Stoffels and colleagues noted that melanoma can metastasize early into regional lymph nodes, making sentinel lymph node excision the most important diagnostic and potentially therapeutic procedure for patients with melanoma. The histological status of the sentinel lymph node is also the most relevant prognostic factor for overall survival in patients with melanoma.
The researchers reviewed a melanoma patient database to identify a group of 464 patients eligible for sentinel lymph node excision between March 2003 and April 2011. Of this group, 403 patients with clinically negative lymph nodes, who underwent sentinel lymph node excision with or without preoperative SPECT/CT, were identified for subsequent analysis.
Between March 2003 and October 2008, 254 patients with melanoma underwent sentinel lymph node excision without preoperative SPECT/CT. Between November 2008 and April 2011, all sentinel node scintigraphies were performed with SPECT/CT, which amounted to 149 cases. Using SPECT/CT allowed sentinel lymph node excision in the head and neck area more frequently (2% for standard imaging, compared with 23% for SPECT/CT).
A total of 833 sentinel lymph nodes were removed from the 403 patients. Stoffels and colleagues found 2.40 sentinel lymph nodes per patient in the SPECT/CT group, compared with 1.87 sentinel lymph nodes per patient in the standard group. Fifty-one (14%) of 358 excised sentinel lymph nodes in the SPECT/CT cohort showed metastatic involvement, compared with 54 (11%) of 475 sentinel lymph nodes in the standard cohort.
The researchers also identified 41 patients (27%) with positive sentinel lymph nodes in the SPECT/CT cohort and 48 patients (19%) with positive sentinel lymph nodes in the standard group. The number of positive sentinel lymph nodes per patient was significantly higher in the SPECT/CT cohort (0.34) than in the standard cohort (0.21).
"The local relapse rate in the SPECT/CT cohort was lower than in the standard cohort (7% versus 24%), which prolonged four-year disease-free survival (94% versus 79%)," the authors noted.
Stoffels and colleagues also found they were able to use smaller incisions in the head and neck area with the additional information from the SPECT/CT scans, as well as alternative entry points due to the exact anatomical localization of the sentinel lymph node.
"The preoperative visualization of [sentinel lymph nodes] with SPECT/CT is technically feasible and facilitates the detection of additional positive sentinel lymph nodes," the authors wrote. "The use of this technique offers the physician the preoperative possibility of determining the exact location and visualization of the [sentinel lymph nodes]."