In a direct comparison between multidetector-row CT (MDCT) and intravascular ultrasound (IVUS), CT was nearly as accurate for detecting both calcified and noncalcified coronary artery plaque, according to a Dutch study presented at the recent RSNA meeting in Chicago.
On a segmental basis, MDCT achieved 96% sensitivity versus IVUS for plaque detection, though it slightly underestimated noncalcified plaque and slightly overestimated calcified plaques, noted researchers from Erasmus University Medical Center in Rotterdam.
Accurate detection and quantification of atherosclerotic plaque -- both calcified and noncalcified -- are needed to improve risk stratification and monitor the progression or regression of disease.
"Currently, IVUS is considered to be the reference method. However, it's an expensive and invasive technique that is not free of complications," presenter Dr. Stella-Lida Papadopoulou said. "Ideally, we need a technique that would be noninvasive and accurately assess atherosclerosis. Under this perspective, the aim of our study was to evaluate the ability of 64-slice CT to detect and quantify atherosclerosis against IVUS."
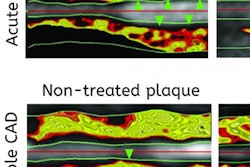
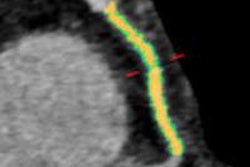
 The MDCT analysis included the normal MDCT image, the MDCT gradient image, and the longitudinal vessel view. Quantitative parameters were determined per 1-mm cross-section and included the lumen area, the vessel area, plaque area, and maximum wall thickness. Plaque was deemed to be present when the wall thickness exceeded 0.5 mm. Regions of interest (ROI) plaque volumes were calculated as the sum of plaque volumes of all the ROI cross-sections. All images courtesy of Dr. Stella-Lida Papadopoulou.
The MDCT analysis included the normal MDCT image, the MDCT gradient image, and the longitudinal vessel view. Quantitative parameters were determined per 1-mm cross-section and included the lumen area, the vessel area, plaque area, and maximum wall thickness. Plaque was deemed to be present when the wall thickness exceeded 0.5 mm. Regions of interest (ROI) plaque volumes were calculated as the sum of plaque volumes of all the ROI cross-sections. All images courtesy of Dr. Stella-Lida Papadopoulou.Both IVUS (44-mHz catheter) and 64-detector-row MDCT were performed in 32 symptomatic patients. The MDCT and IVUS datasets of 44 coronary arteries were coregistered using a newly developed and validated fusion technique that derived quantitative parameters from both imaging modalities using a stepwise approach.
"For analysis of the results, several parameters were compared by section, including lumen area, vessel area, plaque area (vessel area minus lumen area), and maximum wall thickness, defined as the distance between the lumen and the vessel wall," Papadopoulou said. "We considered plaque to be present when the maximum wall thickness was above 0.5 mm." This is criterion commonly used for IVUS but it has not been previously used for CT.
Plaque volumes were calculated for each region of interest (ROI), and the sum of plaque volume cross-sections was calculated according to Simpson's rule, she said.
Compared with IVUS, 64-detector-row MDCT enabled correct detection in 957 of 1,109 cross-sections containing plaque (sensitivity 86%). In 180 of 255 cross-sections, atherosclerosis was correctly excluded (specificity 71%). At the segmental level, MDCT detected 213 of 220 segments with atherosclerotic plaque (sensitivity 96%), while correctly ruling out the presence of any plaque in 28 of 32 segments, for a specificity of 88%.

"We further assessed interobserver agreement and found it moderate (k = 0.51), for cross-sectional level and excellent (k = 1.0) for the segmental level," Papadopoulou said. Detection was also assessed by plaque size. "As plaque gets bigger, the detection rate increases, and for plaques bigger than 1 mm, it's really excellent," she said.
 Plaque detection varied according to plaque size; MDCT was 94% sensitive for detecting plaques larger than 1 mm.
Plaque detection varied according to plaque size; MDCT was 94% sensitive for detecting plaques larger than 1 mm.Detection rate was excellent for plaques larger than 1 mm maximal intimal thickness (94%) and plaques located within the proximal 40 mm from the ostium (> 88%).
"For more distal plaques, sensitivity decreases. However, we found that for plaques located in the proximal 40 mm from the ostium the detection rate was above 88%," Papadopoulou said. "This is important because most clinically relevant plaques are located in the proximal part of the vessel."
 Plaque detection diminished with greater distances from the coronary ostium, with sensitivity greater than 88% for plaques located within the proximal 40 mm of the vessel.
Plaque detection diminished with greater distances from the coronary ostium, with sensitivity greater than 88% for plaques located within the proximal 40 mm of the vessel.The Pearson's correlation coefficient for vessel plaque volumes measured by MDCT and IVUS was r = 0.91 (p < 0.001). Bland-Altman analysis showed a slight nonsignificant underestimation of any plaque volume by MDCT (p = 0.5), with a trend to underestimate noncalcified (p = 0.22), and overestimate mixed or calcified (p = 0.87) plaque volumes.
CT tended to underestimate plaque volumes by approximately 2%. More important, an analysis by plaque composition found that CT underestimated noncalcified plaque volumes by approximately 11%, while plaques containing calcium were overestimated by approximately 4%.
"CT showed good diagnostic accuracy to detect plaque, and we found a good correlation between IVUS and CT for the quantification of plaque volumes," Papadopoulou commented. "Finally, for the very small or distal vessels, coronary plaques were more difficult to assess. The resolution of CT is not as good as IVUS, and specifically very small noncalcified plaques are difficult to assess."
In response to a question from the audience, Papadopoulou said that only one patient was excluded for heavily calcified vessels. The study was targeted at symptomatic patients with mostly mild atherosclerotic disease, she said, and in any case, CT is well established for detecting coronary artery calcium.
The study was recently published in Atherosclerosis (November 2011, Vol. 219:1, pp. 163-170), Papadopoulou said.