Implementing a hybrid iterative reconstruction technique has enabled radiologists at the Technical University of Munich (TUM) to achieve an average dose reduction of about 50% in CT examinations, but they stress the level of dose reduction depends critically on the initial settings, type of examination, and subjective image criteria -- and image quality requires constant evaluation.
Sophisticated image reconstruction algorithms have been developed over the past few years. A key factor has been the significant increase in computing power necessary for image reconstruction algorithms beyond standard filtered back projection (FBP). At the TUM, radiologists have worked on the clinical integration of iDose from Philips Healthcare on a 256-slice multidetector CT unit (Brilliance iCT) to lower radiation dose while retaining an image quality at least equal to standard FBP reconstruction. They presented their findings at the recent RSNA congress.
"Cancer risks associated with CT imaging remain a constant subject of debate. Some authors estimate that 1.5-2% of all cancer risks in the U.S. may be attributable to the clinical use of CT, whereas others argue that data to prove this assumption is lacking," noted Dr. Alexander Fingerle, from the Institute for Clinical Radiology at the TUM.
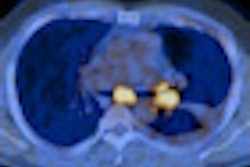
 Left: Filtered back projection images using Brilliance iCT. Scan Parameters: 120 kVp, 73 mAs, 23.7 cm coverage, 3.6 s scan time, 2.3 mSv. Right: Iterative reconstruction using iDose4. Scan parameters: 120 kVp, 33 mAs, 23.7 cm coverage, 3.6 s scan time, 1.2 mSv. This patient was scanned as a follow-up for multiple lesions in the liver and a mass in the abdominal cavity. The original scan was performed at 73 mAs and 2.3 mSv, and the follow-up scan was performed at 33 mAs and 1.2 mSv, without sacrificing image quality.All images courtesy of CMU Shengjing, People's Republic of China.
Left: Filtered back projection images using Brilliance iCT. Scan Parameters: 120 kVp, 73 mAs, 23.7 cm coverage, 3.6 s scan time, 2.3 mSv. Right: Iterative reconstruction using iDose4. Scan parameters: 120 kVp, 33 mAs, 23.7 cm coverage, 3.6 s scan time, 1.2 mSv. This patient was scanned as a follow-up for multiple lesions in the liver and a mass in the abdominal cavity. The original scan was performed at 73 mAs and 2.3 mSv, and the follow-up scan was performed at 33 mAs and 1.2 mSv, without sacrificing image quality.All images courtesy of CMU Shengjing, People's Republic of China.Before the integration of iDose in clinical routine, Fingerle and his colleagues evaluated the algorithm's performance in a preclinical phantom study. They assessed CT number uniformity, low contrast quality, noise characteristics, and spatial resolution. When applying the iDose algorithm to low-dose CT protocol (120kV, 50 mAs), CT numbers were revealed in the level of standard dose FBP reconstructions (120kV, 250 mAs). Calculations of the modulation transfer function with a wire phantom and visual evaluation of the bar pattern of a Catphan 600 phantom showed no decrease in resolution with the use of iDose.
For the clinical evaluation, the researchers performed low-dose CT on cancer patients who had had a previous full-dose examination. The body mass index (BMI) CT protocol was modified so that patients received the next CT scan at one BMI/dose level lower. They obtained a dose reduction of about 50%, while retaining an image quality at least equal to the full-dose examination.
"It is important to note that a simple change to a previous full-dose protocol fitting for all anatomic regions and examination types is not reasonable. For example, with CT angiographies we see the potential for dose reductions of more than 50% with the use of higher iDose levels," Fingerle pointed out.
He explained that the most relevant measures for radiation dose include absorbed dose (energy absorbed per unit of mass in Gray [Gy], 1 Gy = 1 J/kg), CT dose index (CTDIvol, mean dose in scanned volume in mGy, given by CT scanner), dose length product (DLP, length of the scanned volume), organ dose (radiation dose delivered to an organ in mGy), and effective dose (the sum of all weighted organ doses, which allows an approximate of the risk due to radiation exposure in Sievert [Sv], 1 Sv = 1 J/kg).
In Germany, the average exposure to radiation from natural sources like cosmic radiation and radon inhalation adds up to an effective dose of about 2 mSv/a. Also, there is an average radiation exposure of another 2 mSv/a coming from artificial sources, of which the largest part is medical imaging. The average effective does of background radiation is 4 mSv/a.
 iDose cardiac. Dose modulation while still maintaining the noise index. This prospective cardiac scan was performed on a by-pass patient. Multiple areas of calcium were identified in the RCA and LAD.
iDose cardiac. Dose modulation while still maintaining the noise index. This prospective cardiac scan was performed on a by-pass patient. Multiple areas of calcium were identified in the RCA and LAD.Radiation doses from CT studies are typically in the range of 1-20 mSv, depending on region and scan protocol, but doses can easily double, especially in abdominal scan on larger patients. The typical tube voltage setting for a full-dose CT examination in adults is usually between 120 and 140 kVp. Tube voltage settings of 80 kVp are acceptable in pediatric scans, and values of 80-120 kVp are advised for smaller adults. Higher kVp increases photon flux and average photon energy, leading to an exponential increase in radiation dose, according to Fingerle.
Tube current is directly proportional to photon flux, and a doubling of the tube current would increase radiation dose by a factor of two. For multidetector CT scanners, there is no straightforward correlation between pitch and radiation dose. Gantry rotation time is directly proportional to radiation dose.
At the TUM, average radiation dose with CT was already below the 2010 reference values of the Bundesamt fuer Strahlenschutz (Federal Office for Radiation Protection) before the implementation of the reconstruction algorithm. The table below shows the settings for a CT scan of the chest, abdomen, and pelvis. The 2010 DLP reference value for this type of examination is 1,300 mGy/cm.
Settings for a CT scan of the chest, abdomen, and pelvis using a protocol adapted to body mass index (BMI)
|
||||||||||||||||||||||||
| Source: Technical University of Munich |
Standard FBP reconstruction is unable to guarantee diagnostic image quality when lowering radiation dose in CT due to an inherent increase in image noise, and iterative reconstruction algorithms have been developed as an alternative to FBP. Reconstruction based on these algorithms used advanced mathematical models to decrease image noise and remove artifacts with lower tube currents, concluded Fingerle.