Contrast-enhanced ultrasound (CEUS) is the most sensitive method for detecting even minor blood flow in the bowel, which is a relevant sign for inflammatory bowel disease (IBD). In terms of resolution, CEUS is a more powerful tool than ultrasound alone for characterization of inflammatory masses.
This is the view of Dr. Stephanie Wilson, a clinical professor of radiology at the University of Calgary in Canada. The use of contrast agents in detecting IBD can make a very positive contribution to patient management when the activity of the disease is uncertain in an identified loop of thickened bowel, as may be the case when the loop is deep in the abdomen or the signals of blood flow -- shown by Doppler sonography -- are too weak, she noted.
"Contrast agents are also beneficial in the resolution of an inflammatory mass as is frequently shown on imaging studies of those with IBD. While the grayscale features of abscess and phlegmon may be specific, there are many instances when this distinction cannot be made with conventional ultrasound alone. The injection of a microbubble contrast agent will show diffuse enhancement of an inflammatory phlegmonous mass, whereas an abscess will be avascular in the regions where there is pus," said Wilson, who will present on this topic during the opening day of the World Federation for Ultrasound in Medicine and Biology (WFUMB) congress, to be held in Vienna from 26 to 29 August.

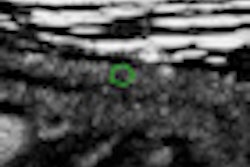
 Cross-sectional (left) and longitudinal (right) images of the terminal ileum show thickened bowel wall and inflammatory echogenic fat in a young female patient with acute Crohn's disease of the terminal ileum. All images courtesy of Dr. Stephanie Wilson.
Cross-sectional (left) and longitudinal (right) images of the terminal ileum show thickened bowel wall and inflammatory echogenic fat in a young female patient with acute Crohn's disease of the terminal ileum. All images courtesy of Dr. Stephanie Wilson.Elastography can play a role in the differentiation of a fibrotic from an inflammatory stricture in IBD, she explained. Furthermore, the use of volumetric techniques now makes it possible to scan in 3D and 4D, and to show volumes of data rather than a simple 2D display.
IBD is a group of inflammatory conditions of the colon and the small intestines. Crohn's disease (CD) and ulcerative colitis (UC) are the two most common forms of IBD. Although the disease shows immunity alteration and dysbiosis in development, there is no known etiology or cure. In most cases onset is in adolescence or young adult life, and up to 80% of patients with CD have to face surgical bowel resection at some point due to complications such as stricture and mechanical bowel obstruction.
Imaging of the abdomen plays a major role in detecting IBD and in its surveillance, according to Wilson. "Without therapy, the disease has a natural tendency for a remitting and relapsing course. As neither clinical symptoms nor inflammatory markers are reliable predictors of disease activity, there is a huge demand for imaging of the bowel to show the disease extent and activity, and to monitor progression and response to therapy. Current popular therapies are aimed at mucosal healing and alteration of the natural course of the disease."
The gold standard in diagnosing IBD is still colonoscopy, where morphology and biopsy provide information about the patient's condition. Ultrasound is also a very efficient way to detect IBD and is as accurate in terms of results as MRI and CT. Aside from being accurate in detecting the disease, there are also other good reasons why ultrasound should be the preferred method to examine patients with known or suspect IBD.
"Excessive radiation exposure from overuse of CT scans is now a well-recognized outcome in this population. Furthermore, while highly valuable, colonoscopy is invasive and no patient will tolerate anything other than occasional repeat examinations, emphasizing the need for noninvasive and accurate imaging techniques. Ultrasound has excellent spatial resolution allowing for visualization of all of the layers of the bowel wall," she said.

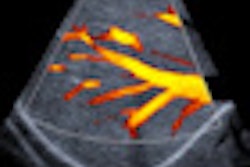
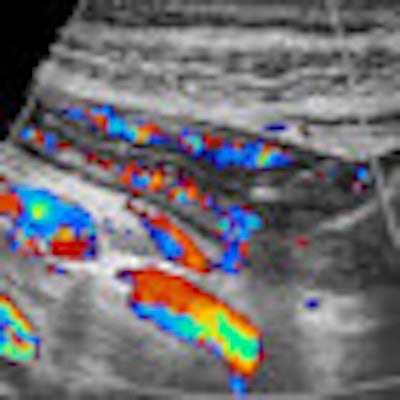
 Additional color Doppler images show hyperermia of the bowel.
Additional color Doppler images show hyperermia of the bowel.When performing ultrasound of the gastrointestinal tract, there are technical and patient-related challenges. The technical demands include equipment requirements for a broad range of transducer frequencies to allow for scanning of the bowel within the focal range of the transducer so that exceptionally high resolution can be achieved. Although all ultrasound machines have low-frequency probes available, it is the addition of high-frequency probes, both linear and convex, which allows for good bowel assessment, especially in thin patients.
In addition to these technical configurations, the ultrasound equipment must be capable of creating dynamic real-time movie files to show the global perspective of the disease, as well as peristalsis of the bowel. Doppler ultrasound is an essential basic tool as blood flow within the bowel is a possible sign of inflammation.
The few patient-related challenges include morbid obesity, peristalsis, and gas. In general terms, excellent assessment of the gastrointestinal tract can be carried out with ultrasound in most patients. Specific skills also are required on the part of the sonographer.
"Reliable performance of good ultrasound examinations of the bowel requires a dedicated and skilled sonographer. Although the examinations are not so difficult, a high skill level is required to detect the subtleties of the sonographic features of disease and their complications. Sonography of the bowel is not for the faint of heart, nor for dabblers."
David Zizka is a communications specialist at the European Society of Radiology's (ESR) press office.
Note: This article was originally published in the WFUMB newsletter.