Researchers in Japan have developed computer-aided detection (CAD) software that detects lung nodules in PET/CT images of lung cancer screening patients. Applying a combined CAD system to both modalities instead of CT or PET alone nearly doubled the number of solitary pulmonary nodules (SPNs) detected.
The software could make a contribution to cancer screening in Japan, which is ramping up in a big way in the country. The researchers believe that CAD could overcome the blind spots that inhibit their visualization with either modality alone, and detect cancer earlier, which is key to improving survival rates.
"To reduce cancer-related deaths it is essential to detect cancer at an early stage," said Atsushi Teramoto, PhD, from Fujita Health University in Toyoake, Japan. "CT is widely used to detect early lung cancers. Some Japanese and Korean hospitals are starting to acquire PET/CT exams for screening of cancer."
In 2009, approximately 22,000 patients underwent whole-body PET/CT in three large programs in Japan, Teramoto told AuntMinnie.com. About 30% of the total cancers detected at PET/CT are lung cancer, he said.
In most places, of course, CT is the most common modality used to screen for lung cancer specifically. And while lung CAD applications remain mostly investigational, they have proved their worth in lung cancer screening, where following ever-growing numbers of patients and lung nodules for longer periods of time make for very difficult workloads.
Whatever the reading paradigm, CAD finds lung cancers that radiologists -- even groups of radiologists -- can miss. But a lot of negative lung screening images need to be read before a single positive case is found.
"In PET/CT screening, cancer is found from 2% of the examinations, so 98% are normal cases," Teramoto said in a talk at the 2010 Computer Assisted Radiology and Surgery (CARS) meeting in Geneva. "It is very difficult to find the cancers."
But CT alone -- and, therefore, CAD systems based on CT alone -- has blind spots that hide some potential cancers, which is why screening programs in Asia are increasingly adopting PET/CT despite its higher relative cost, Teramoto said.
"PET/CT is very expensive, but I believe it will possibly be used as general screening tool," he said.
The investigational lung CAD system built by Teramoto, Naoki Hayashi, Hiroshi Fujita, PhD, Tsuneo Tamaki, MD, and colleagues from Fujita Health and Gifu University in Gifu, Japan, detects lung nodules visualized on both the CT and PET data and combines them.
"The CT part detects SPN and the PET looks for high uptake regions," he said. In combination, both anatomic and functional images are obtained.
The application was tested on 20 cancer screening patients from Nagoya Radiological Diagnosis Foundation in Nagoya, Japan, which has scanned about 10,000 patients with PET/CT in the past year, 10% of which were for general cancer screening, Teramoto said.
CAD under the hood
In the CT images, the lung region is detected and nodules are enhanced using a cylindrical filter the group designed to speed up processing, Teramoto explained.
Image processing is extremely slow using standard 3D enhancement for solitary pulmonary nodules, he said. The cylindrical filter developed for the CAD scheme avoids much of the computational burden by simply measuring, then outputting, the difference in pixel values between the maximum value of a cylindrical kernel and the center pixel.
Computation time is reduced because the cylindrical kernel can be replaced by a ring kernel in a maximum intensity projection (MIP) CT image. The cylinder reduces processing times tenfold compared to traditional 3D methods, Teramoto said.
"After enhancing the nodule, it is binarized using a threshold to distinguish candidate lesions from the background, and then candidate lesions are obtained using 3D labeling," he said.
The PET side of the CAD system uses the CT images to determine the region to be analyzed. Images are binarized based on a predetermined uptake threshold of 2.0 standardized uptake value to distinguish the high-uptake regions. Finally, detection results from CT and PET are combined to obtain the candidate lesions -- along with a lot of false positives.
"We reduced the false positives using characteristic features and support vector machines [SVMs]," Teramoto said. The SVM uses seven nodule characteristics, including area, volume, surface area, diameter, CT value, concentration index, and compactness, to distinguish true- from false-positive detections.
 |
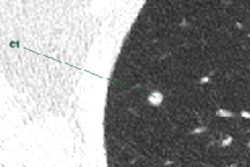
| A nodule missed by PET/CT CAD in the PET images due to low radiotracer uptake was readily detected at CT. All images courtesy of Atsushi Teramoto, PhD. |
 |
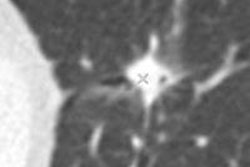
| A large nodule near the mediastinum was obscured on CT images but readily detectable on PET. |
Improved detection in patients
To evaluate the system's utility in clinical images, the group applied it to the PET/CT scanning results from 20 lung cancer screening patients in Nagoya. All patients were scanned using a Biograph TruePoint PET/CT scanner (Siemens Healthcare, Erlangen, Germany), and the images were reviewed by experienced radiologists, who found a total of 29 nodules in 14 patients, along with six normal cases.
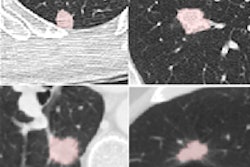
Of the 29 solitary pulmonary nodules found by the radiologists, two ground-glass opacities remained undetected on CAD by either PET or CT, including one located adjacent to a blood vessel and a second attached to the chest wall. Visualization on CT was impaired by the nodules' location, while PET "had a low uptake value," Teramoto said.
According to the results, CT demonstrated a true-positive fraction of 55% (16/29 nodules), compared with 59% (17/29 nodules) for the PET portion of the scan.
"In combination, the [true-positive fraction] was 93% -- this indicates that PET/CT detection was more valuable than PET or CT detections" alone, Teramoto said. Most false positives were located at curves in the blood vessels, he added.
|
||||||||||||
| True-positive fraction (TPF) shows that the combination of PET and CT nearly doubled the detection sensitivity of either method alone. Data courtesy of Atsushi Teramoto, PhD. |
The CAD scheme improves upon the results typically obtained by examining independently acquired PET and CT scans as well, Teramoto said. The challenge is the large number of images that must be examined -- about 1,000 just for a whole-body PET scan, he said.
Future efforts will focus on better detection of false positives and ground-glass nodules.
By Eric Barnes
AuntMinnie.com staff writer
August 6, 2010
Related Reading
Lung cancer often recurs more than 5 years after resection, July 19, 2010
PET/CT beats CT in NSCLC staging, but both have limitations, July 2, 2010
CT method measures airway calcium to diagnose lung cancer, June 28, 2010
Chest x-ray CAD offers value in detecting lung cancers, June 18, 2010
CARS report: New CAD tool follows lung nodules over time, June 30, 2009
Copyright © 2010 AuntMinnie.com