In a study that probes what may be the largest database of detailed coronary CT angiography (CTA) results assembled to date, New York City researchers found an integral association between coronary artery disease and mortality at coronary CTA in patients without known heart disease.
For the team from Weill Cornell Medical College and eight collaborating institutions, however, 10,000 patients is only the beginning. Even as data analysis begins in earnest and patients continue to be followed, the group is actively recruiting more cardiac imaging centers to join its new CONFIRM (Coronary CT Angiography Evaluation for Clinical Outcomes) registry.
Principal investigator James Min, MD, from Weill Cornell University Medical Center, presented the first results earlier this month at the Society of Cardiovascular Computed Tomography (SCCT) meeting in Las Vegas.
The researchers analyzed data from more than 10,000 patients who underwent coronary CTA for suspected coronary artery disease (CAD). In a little more than two years of follow-up, the results showed that the risk of death grew in step with the number of arteries affected, as well as the significance of the obstruction.
"In a large international, multicenter cohort, I think we have definitively established the prognostic value of coronary CTA findings in patients without known coronary artery disease," Min told AuntMinnie.com in a telephone interview.
Min and colleagues evaluated coronary CTA data from 10,062 consecutive patients (54% men) with suspected coronary artery disease.
In a departure from earlier large-scale analyses that took all comers, this study examined only data that was acquired on 64-detector-row scanners, and the researchers expressed the results both by patient and by coronary artery segment.
"Most patients presented with chest pain -- 50% presented with typical or atypical angina and 50% with noncardiac pain including dyspnea," Min said.
The researchers calculated all-cause mortality in 241 (2.4%) of the patients during the follow-up period (2.2 years ± 1.0) in relation to the extent and severity of coronary artery disease. Specifically, they considered the presence of any coronary artery disease as well as obstructive stenoses 50% or greater in increasing numbers of major epicardial vessels.
At follow-up of patients presenting for 64-detector-row coronary CTA, Min and his team found mortality of 0.98% (31/3,156) among patients with no plaque at CTA, 1.8% (71/3,859) for patients with nonobstructive CAD, and 4.0% (119/3,006) for patients with obstructive CAD.
Mortality rose in a stepwise fashion among patients with obstructive CAD, increasing in relation to the number of vessels involved, as shown in the table below:
|
||||||||||||||||
| CI = confidence interval. Data courtesy of James Min, MD. |
Cox regression and risk-adjusted analyses showed a progressively increased risk of mortality with each increase in the number of affected vessels and the severity of disease in each vessel, compared to individuals with no plaque.
 |
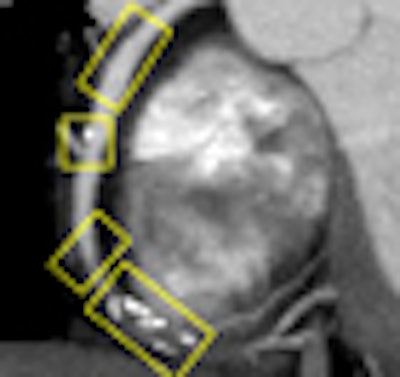
| Maximum intensity projection (MIP) image of the right coronary artery depicting normal, mild, moderate, and severe coronary artery stenoses. Images courtesy of James Min, MD. |
 |
| Unadjusted Kaplan-Meier survival curves depict mortality in relationship to extent and severity of coronary artery disease. |
Obstructive CAD accurately identifies individuals at increased risk for all-cause mortality, he said. As a corollary, the absence of obstructive CAD on coronary CTA scans identified patients at very low risk of death, in numbers consistent with but larger than previous studies.
"We established that coronary CTA is prognostic in that it allows for risk stratification at the per-patient and per-segment levels, which I think is an important thing," Min said. "Using a 16-segment [American Heart Association] model, it turns out that every additional segment that has coronary artery disease connotes an 11% increased risk of death during the two-year follow-up period."
Bigger and better
The early results inaugurate a study that aims to follow large numbers of patients over long periods of time, said Min. The existing patients continue to be followed as new ones are added.
The database is "locked" each time the analytical process begins on the sum of patients accrued to date, he said. The current research database is locked at more than 12,000 patients.
"Our hope is that we'll continue to accrue more and more patients and continue to follow them out for longer and longer periods of time," he said. "There are several other sites that have expressed interest in contributing to this registry."
The analyses will study everything from which vessels and segments have the greatest effect on future events, to the most effective way to report the results.
"Whether or not to report coronary artery disease by the number of vessels with obstructive disease, whether or not to perform a weighted assessment that includes nonobstructive disease, whether to include plaque composition, whether to include coronary CTA findings on top of coronary calcium findings -- we're examining all these things," he said.
At the same time, there are no illusions that the best way to analyze the data will be obvious or easy.
"It's not going to be as simple as we think it is," he said. "We're going to have to identify all of the prognostic factors and determine which ones are independently associated with adverse prognoses," Min said. But the cooperative spirit of the team and the quality of the data each center have contributed has made the work "a pleasure," he said.
Collaborating institutions in the CONFIRM registry include the University of Erlangen, Erlangen, Germany (Stephan Achenbach, MD, et al); Henry Ford Medical Center, Detroit (Mouaz Al-Mallah, MD, et al); Cedars-Sinai Medical Center, Los Angeles (Daniel Berman, MD, et al); Harbor UCLA Medical Center, Los Angeles (Matthew Budoff, MD, et al); Tennessee Heart and Vascular Institute, Nashville (Tracy Callister, MD, et al); Yonsei University, Seoul, Korea (Hyuk-Jae Chang, MD, et al); Ottawa Heart Institute, Ottawa, Canada (Benjamin Chow, MD, et al); Capital Cardiology Associates, Albany, NY (Augustine Delago, MD, et al); University of Munich, Munich, Germany (Jörg Hausleiter, MD, et al); Cardiovascular Medical Group, Los Angeles (Ronald Karlsberg, MD, et al); University Hospital, Zurich, Switzerland (Philipp Kaufmann, MD, et al); and Emory University School of Medicine in Atlanta (Leslee Shaw, MD, et al).
By Eric Barnes
AuntMinnie.com staff writer
July 30, 2010
Related Reading
Cardiac model favors treadmill then CTA for low-risk patients, June 7, 2010
Cardiac CAD safely rules out coronary artery disease, June 1, 2010
Zero calcium score enough to send chest pain patients home, February 10, 2010
Analysis favors coronary CTA over stress MPS for chest pain, January 15, 2010
ACCURACY trial compares coronary CTA to angiography, January 18, 2008
Copyright © 2010 AuntMinnie.com