A new computer-aided detection (CAD) algorithm goes beyond flat-polyp detection to find submucosally invading colorectal cancers with virtual colonoscopy (also known as CT colonography).
Researchers from London-based CAD developer Medicsight say the new software (ColonCAD 4.0) offers an important alternative to traditional CAD feature classification that could improve the sensitivity of all virtual colonoscopy studies.
Colorectal cancer arises in a pre-existing adenoma or normal mucosa, and it necessarily goes through a stage known as "colorectal carcinoma with a submucosal invasion" (CCSI), explained Medicsight employee Greg Slabaugh in a presentation at the 2009 International Symposium on Virtual Colonoscopy.
"CCSI lesions destroy the mucosa, invade the submucosal layer, and are likely to develop into advanced carcinomas," Slabaugh said. "The submucosal layer consists of loose tissue including lymphatic or venous vessels. We believe that CCSI lesions are clearly important for early diagnosis. It is therefore important to utilize CAD against CCSI lesions and reliably detect them in CTC examinations."
 |
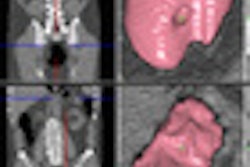
| Above, schematic image of a submucosally invading CCSI shows the lesion penetrating the mucosal layer and going into submucosal layer. Below, histopathological view of CCSI lesion. All images courtesy of Greg Slabaugh and Medicsight. |
 |
The study evaluated the performance of a new CAD algorithm for its ability to detect submucosally invading lesions in diagnostic CTC data. ColonCAD 4.0 was released internationally in 2009 but has not yet been approved by the U.S. Food and Drug Administration (FDA), he added.
The new software wasn't designed to find the subtle submucosal lesions at VC -- it simply turned out to be pretty good at detecting them, Slabaugh said. In fact, the CAD algorithm was "trained" on normal VC images that did not exhibit submucosal invasion, and the developers were careful to separate the training data from the testing data used to evaluate CAD's performance, he said.
The CAD algorithm's five-part process includes the following:
- Colon segmentation using adaptive thresholding and mathematical morphology. This function finds the threshold between air and tissue per CT values to separate the colon from other structures, analyzing each axial image slice and grouping objects into 3D regions.
- Candidate generation looks for raised objects protruding into colon lumen. It was designed to be as sensitive as possible and, therefore, can include high numbers of false positives.
- Feature calculation characterizes potential colorectal lesions based on statistical measures of CT values, shape, volume, etc.
- Classification reduces the number of lesion candidates based on statistical features derived from the images. The process is designed to preserve as many true-positive findings as possible, while eliminating as many false positives as possible.
- Results can be varied by adjusting the operating point of the classifier to provide, for example, higher sensitivity at the expense of more false-positive results.
Thirty diagnostic CTC patients, each exhibiting submucosal invasion, were scanned at Japan's National Cancer Center in Tokyo using a 64-detector-row CT scanner (Aquilion, Toshiba Medical Systems, Otawara, Japan) in both prone and supine positions following cathartic bowel cleansing and colonic insufflation. Scanner settings included 120 kVp, 150-200 mAs with automated exposure control, and 0.5-mm slice thickness. Two expert radiologists examined the images.
The presence and location of all lesions were confirmed with optical colonoscopy and histopathologic analysis from surgical specimens, Slabaugh said. Lesion sizes varied from 7-55 mm (mean, 25 mm). Detection analysis was limited to additional submucosally invading lesions found with the use of the CAD algorithm and confirmed at colonoscopy, Slabaugh noted.
At the default operating point for the software, the CAD system produced an overall per-lesion sensitivity of 76.6% (23/30) for detecting submucosally invading lesions, with an average of 5.8 additional findings beyond what the radiologists saw for each patient.
 |
| True-positive results were typically raised lesions characterized by granular or carpetlike morphology. |
When the CAD's operating point was increased to maximize sensitivity, it achieved an overall per-lesion sensitivity of 86.7% (26/30) for detecting submucosally invading lesions, with an average of 15.5 additional findings per case beyond what the two expert readers saw. Additional CAD findings not associated with submucosal lesions were excluded from the sensitivity analysis.
 |
| False-negative results tended to be flatter lesions, or those located on haustral folds. |
The system's successful detection of slightly raised submucosal lesions "should hardly come as a surprise based on the way we do candidate generation," Slabaugh said. "Raised lesions were characterized by granular or carpetlike morphology, while [CAD] false negatives tended to be flatter."
Other false negatives were subtle lesions located on haustral folds, he said.
"Our CAD system was used to evaluate performance on submucosal lesions, and we believe it is effective for their detection," Slabaugh said.
The results also demonstrate the potential for improved lesion detection at alternative classifier operating points -- for example, adjusting the classifier to maximize detection sensitivity at the expense of additional false-positive results. Overall, the few false negatives were characterized by flatter morphology, he said.
For the future, "we're quite interested in adapting the algorithm to the submucosal lesion for enhanced performance, and, furthermore, we really want to do a training algorithm on CCSI lesions to get optimal performance," Slabaugh said.
By Eric Barnes
AuntMinnie.com staff writer
February 4, 2010
Related Reading
VC screening effective in Medicare-age screening cohort, January 27, 2010
VC CAD nabs undetected polyps in jumbo screening study, October 29, 2009
Readers undaunted by VC CAD false positives, June 12, 2009
VC CAD plus 3D improves sensitivity for novice readers, April 21, 2009
VC CAD plus electronic cleaning boosts sensitivity, false positives, April 10, 2009
Copyright © 2010 AuntMinnie.com