A simulation study evaluating the quality of whole-body PET/MR images of pediatric cancer patients shows the amount of PET tracer administered can be significantly reduced while still obtaining diagnostic quality images. Researchers from the University of Tübingen in Germany, who have been investigating the feasibility of using PET/MRI in lieu of PET/CT, developed and validated a methodology to accurately create low-activity PET images from previously acquired PET scan data.
The approach could allow radiologists to define optimal tracer doses for PET/MRI procedures on a patient-by-patient basis.
For any PET exam, a trade-off exists between radiation dose exposure to a patient and the diagnostic quality of the acquired images. Because it is unethical to subject a patient to multiple exams of different tracer doses, lead author Sergios Gatidis, of the department of radiology's diagnostic and interventional section, and colleagues developed a method for simulating low-dose PET images. The resulting images enable direct comparison of different tracer doses in a single patient.
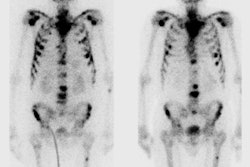
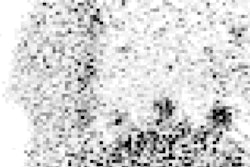
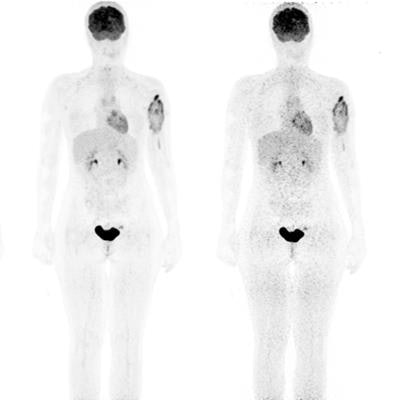
 FDG-PET/MRI of a 16-year-old girl with osteosarcoma of the left humerus. A simulated tracer activity of 1.5 MBq/kg shows good diagnostic PET quality comparable with the originally injected activity of 2.9 MBq/kg. Further reduction to 0.25 MBq/kg results in markedly reduced PET image quality. The right panel shows fusion of PET and coronal MR images.
FDG-PET/MRI of a 16-year-old girl with osteosarcoma of the left humerus. A simulated tracer activity of 1.5 MBq/kg shows good diagnostic PET quality comparable with the originally injected activity of 2.9 MBq/kg. Further reduction to 0.25 MBq/kg results in markedly reduced PET image quality. The right panel shows fusion of PET and coronal MR images.In earlier studies, the authors showed that radiation exposure could be reduced by up to 70% by replacing PET/CT with PET/MRI using the tracer F-18 FDG (FDG). In a study of 18 pediatric cancer patients with solid tumors, they determined PET/MRI and PET/CT achieved similar lesion detection rates, with MRI data from areas of soft tissue providing additional diagnostic information that could not be seen on CT. A subsequent study showed FDG-PET/MRI without contrast was technically feasible, and at least equivalent to FDG-PET/CT, for tumor staging and characterization in patients under the age of 6.
In this latest study, the authors assessed the feasibility of reducing radiation exposure from the PET portion of the PET/MRI scan (European Journal of Nuclear Medicine and Molecular Imaging, 26 August 2016).
Simulation study
The simulation methodology allows reconstruction of PET images with equivalent properties to PET images measured after injection of lower tracer doses. The use of randomized subsampling of PET data enables more realistic clinical dose simulations incorporating dynamic measurement effects, such as tracer uptake for longer measurements, decay of short half-life tracers, and/or patient movement.
The researchers simulated different tracer activities (0.25 MBq/kg FDG to 2.5 MBq/kg) using data from 30 whole-body FDG-PET/MRI exams of 24 pediatric patients diagnosed with or suspected of having solid tumor malignancies. A pediatric radiologist and a nuclear medicine physician analyzed the PET data independently. They assessed the visual detectability of physiologic FDG uptake in 19 anatomic structures and the detectability of potentially pathologic focal FDG uptake in other parts of the body, classifying all findings considered relevant to an oncologic diagnosis. The readers specified the lowest level of tracer activity simulated that had sufficient image quality. False-positive findings were also calculated.
Study results showed that 88% of datasets with a simulated activity of 1.5 MBq/kg FDG, using point spread function (PSF) reconstruction, had sufficient image quality for accurate interpretation. The use of PSF modelling significantly improved the detection of focal FDG-avid lesions. Lesion detectability and SUV quantification were not relevantly impaired down to simulated tracer activities of 1.5 MBq/kg FDG.
Because current international guidelines for FDG application in pediatric oncology recommend tracer activities of 3 MBq/kg FDG to 5 MBq/kg FDG, this represents a reduction of radiation dose of more than 50%. However, the authors note this may not be feasible for all scans ordered, for example, assessing response to treatment of Hodgkin's lymphoma. Radiologists need to determine optimal tracer levels for each individual patient, based on patient characteristics and the clinical question to be answered.
Gatidis and colleagues point out that even greater reduction might be possible with longer image acquisition time. The original PET image acquisition took four minutes per bed position, instead of the more commonly used two to three minutes. They suggest it is worth investigating a five minute per position acquisition to determine whether tracer activity could be lowered further, noting the additional exam time needed would not exceed the time to perform the MRI scan.
Benefit to cancer survivors
Multiple studies have shown that children who survive pediatric cancer into adulthood and middle age have a higher risk of developing additional cancers or serious medical conditions, as a result of cumulative radiation exposure from radiotherapy and/or routine imaging follow-ups.
A 2008 study estimating cumulative radiation dose from PET/CT scans ordered for diagnosis, staging, and follow-up in 78 cancer patients ages 1 to 18 determined the average cumulative radiation dose was 64.4 mSv for CT (with a range of 2.7 mSv to 326 mSv) and 14.5 mSv for PET (with a range of 2.8 mSv to 73 mSv). This did not include dose from radiotherapy, which almost half of pediatric cancer patients receive. Reducing radiation exposure from any source is of critical importance.
© IOP Publishing Limited. Republished with permission from medicalphysicsweb, a community website covering fundamental research and emerging technologies in medical imaging and radiation therapy.