Despite a short scan length and relatively small dose length product (DLP), contrast-monitoring scans can account for 27% of the overall breast dose accrued from a CT pulmonary angiography (CTPA) study, according to Irish researchers. A small tweak to the kilovoltage (kV) can significantly reduce radiation dose to the breast, they noted.
The researchers conducted a single-center study to compare breast radiation dose in pregnant and nonpregnant women undergoing either a reduced 80-kV contrast-monitoring CTPA protocol or the conventional 120-kV protocol. The team, led by Dr. David P. Mitchell from the radiology department at Mater Misericordiae University Hospital in Dublin, found decreasing the default peak kV resulted in an 88% and 79% reduction in monitoring scan breast dose for pregnant and nonpregnant patients, respectively (European Journal of Radiology, 8 November 2016).
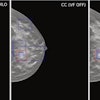
 Above: Axial CT image of the midthorax from a CTPA monitoring scan (bolus-tracking 80-kV technique). The region of interest is centered over the pulmonary trunk and measures 305 Hounsfield units, which is sufficiently high to trigger the diagnostic scan. Below: A scout topogram from the same CTPA study. The transverse line illustrates the level at which the monitoring scan was performed and demonstrates that repeated scanning at this level would increase breast organ dose. All images courtesy of Dr. David P. Mitchell.
Above: Axial CT image of the midthorax from a CTPA monitoring scan (bolus-tracking 80-kV technique). The region of interest is centered over the pulmonary trunk and measures 305 Hounsfield units, which is sufficiently high to trigger the diagnostic scan. Below: A scout topogram from the same CTPA study. The transverse line illustrates the level at which the monitoring scan was performed and demonstrates that repeated scanning at this level would increase breast organ dose. All images courtesy of Dr. David P. Mitchell."Contrast-monitoring techniques are often considered to be minor, if not negligible, contributors to radiation dose, but, in fact, the monitoring scan has a disproportionate effect on breast dose due to its repeated imaging directly over the breasts and the tendency of monitoring scans to be repeated," Mitchell wrote in an email to AuntMinnieEurope.com. "The protocol optimizations required enact significant dose reductions that can be carried out in any radiology department, without compromising diagnostic CTPA quality."
CTPA and dose
CTPA is the current standard of care for detecting pulmonary embolism (PE) in the nonpregnant population. Significant recent improvements have been made in CT technology, but radiation exposure to the breast during CTPA remains a concern, especially for young female patients, according to the researchers.
"In fact, it is mainly due to concerns with breast dose that lower limb venous ultrasound and/or perfusion scintigraphy, rather than CTPA, have been advocated as preferred investigations in the pregnant patient suspected of having a PE," the authors wrote. "While the debate on the best investigation in pregnancy continues, it is important that when the CTPA technique is used, it is optimized with regard to radiation dose."
Patient dose can be reduced in several ways, but they are directed at the diagnostic component of the CTPA study. A typical CTPA study comprises three components: a patient topogram, a contrast-monitoring scan, and a diagnostic scan. The role of the contrast-monitoring scan is to determine the optimum timing between the injection of contrast material and CT data acquisition to obtain adequate pulmonary arterial contrast enhancement, the researchers noted.
"In practice, the contrast-monitoring component entails the continuous imaging of the pulmonary trunk after contrast injection has begun, which can either trigger the diagnostic scan at a predetermined Hounsfield level (i.e., bolus tracking) or can be used to accurately time a separate diagnostic study (i.e., test-bolus timing)," they wrote.
Contrast-monitoring techniques contribute little to the total DLP, but due to the short scan length, the technique does require repetitive scanning through breast tissue when monitoring the pulmonary trunk.
Mitchell and colleagues hypothesized that contrast-monitoring techniques are significant but underappreciated contributors to breast dose during CTPA exams, and, if optimized, they could significantly reduce breast dose without compromising the quality of the diagnostic scan.
The researchers retrospectively studied 221 women undergoing a reduced 80-kV contrast-monitoring CTPA protocol compared with 281 patients using the conventional 120-kV protocol (Somatom Definition AS+, Siemens Healthineers). They analyzed 99 pregnant patients separately.
They found the contrast-monitoring component of a CTPA study constituted 27% of the overall breast dose when using a standard 120-kV protocol compared with only 7% of the overall breast dose in the 80-kV study group. The breast dose from the contrast-monitoring component alone was reduced by 79% in the nonpregnant patients (0.36 mGy ± 0.37 versus 1.7 mGy ± 1.02) and by 88% in the pregnant population (0.25 mGy ± 0.67 versus 2.24 mGy ± 1.61). They found no statistical difference in CTPA diagnostic quality or timing.
"The results of this study demonstrate that conventional CTPA contrast-monitoring techniques account for a quarter of the total breast dose of a CTPA study using modern scanners and iterative reconstruction," the authors wrote. "The impact of these techniques on breast dose is often overlooked due to their very short scan length and thus small contribution to DLP."
However, Mitchell noted different vendors and updated CT protocols may automatically match the kV of the monitoring scan to the diagnostic scan kV, but at present most CT scanners do not seem to match the monitoring scan if a lower kV -- 80 kV, for example -- diagnostic scan is used.
"Our CTPA breast dose data in pregnant patients will be especially relevant because this is a current topic of controversy," Mitchell wrote. "Current international guidelines favor perfusion scintigraphy over CTPA in pregnant women, which is partly due to the relatively high CTPA breast doses quoted in the literature. We believe that the breast doses of 10-70 mGy cited in many guidelines are misleading when compared with an average breast dose of 5 mGy in our study using our reduced dose protocols."