A controversial French-led study published this week has found screening mammography's benefits have been overestimated due to unconventional statistical methods, but screening advocates have been quick to stress the authors have ignored numerous publications proving the efficacy of screening.
The study in question was published in the Journal of the Royal Society of Medicine (JRSM) on 7 July. Having reviewing several randomized trials, lead author Dr. Philippe Autier, an epidemiologist at the Strathclyde Institute of Global Public Health at International Prevention Research Institute (iPRI) in Lyon, said the overestimation results from the use of an unconventional statistical method that differs from that used for other cancer screening trials.
 Dr. Philippe Autier.
Dr. Philippe Autier."Contrary to expectations, numerous studies in North America, Europe, and Australia have shown that the rates of advanced breast cancer have not declined in countries where most women regularly attend mammography screening," he stated in a press release. "Other studies have shown that declines in breast cancer mortality were the same in countries that implemented mammography screening at the end of the 1980s as those that did so 10 to 20 years later. The absence of differences in mortality reductions could not be explained by differences in access to modern therapies."
Dr. Stephen Duffy, from the Wolfson Institute of Preventive Medicine in London, along with Dr. László Tabár from Falun University Hospital in Sweden, heartily disagree with Autier and colleagues' conclusions and maintain there is considerable evidence of an effect of mammography in reducing advanced cancer rates and, therefore, reducing deaths from breast cancer.
Faulty methodology
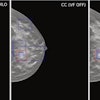
Autier and co-authors evaluated five mammography screening trials conducted in Sweden between 1977 and 1996: Malmö I, Malmö II, Ostergötland, Stockholm, and Gothenburg.
"Breast screening trials were initiated at a time when there was limited experience for designing, conducting, and analyzing cancer screening trials," they wrote. "We, therefore, postulate that the contrasts between breast and cervical or colorectal cancers could be due to differences in the way randomized trials were conducted and analyzed."
To test this, they re-examined the mortality data used and the way risks of breast cancer death were computed in Swedish trials in the light of study design and statistical analyses performed in screening trials on cancers other than breast cancer.
For each trial, they identified the intervention period, when screening was offered to screening groups and not to control groups, and the postintervention period, when screening (or absence of screening) was the same in screening and control groups. Then they determined which cancer deaths had been used for the computation of relative risk of cancer death.
Unconventional computation of the relative risk of breast cancer death affected the reported results of the Swedish trials on mammography screening, which led to an intrinsic bias in favor of screening, they concluded.
Relative risk calculations used deaths due to breast cancers found during intervention periods, but deaths due to breast cancer found at first screening of control groups were added to these groups. After reallocation of the added breast cancer deaths to postintervention periods of control groups, relative risks of 0.86 were obtained for cancers found during intervention periods and 0.83 for cancers found during postintervention periods, indicating constant reduction in the risk of breast cancer death during follow-up, irrespective of screening.
"If calculations of relative risks had been carried out using similar methodological approaches to other cancer screening trials conducted in the more recent era, the Swedish trials would not have found a 20% reduction of breast cancer death due to mammography screening," Autier and colleagues wrote.
In fact, if the Swedish trials had used similar statistical analyses to other cancer screening trials, reductions in the risk of breast cancer death associated with mammography screening would have been much smaller, probably less than 10%, they added.
Advocates chime in
The randomized trials show a considerably greater reduction than 10%, Duffy stated in an email to AuntMinniEurope.com.
"It seems to me that it is more reasonable to consider the actual effect observed in experimental studies than the effect that some commentators feel should have been observed on the basis of observational, ecological results," he wrote.
 Dr. László Tabár.
Dr. László Tabár.Tabár points out that the JRSM article ignores two important studies that were published recently: one from the New England Journal of Medicine that found breast cancer screening reduces mortality by 40%, and another from Norway that found breast cancer screening reduced mortality by 20% to 30% for women ages 50 to 69, followed to age 79, when compared with no screening.
Autier and colleagues' study -- and others like it -- "consistently apply methodology and logic that have (also, consistently) been demonstrated to be biased by confounding, and they have selectively criticized trials (specifically the trials that show a benefit from screening) as biased, without acknowledging (or rebutting) the literature that confronts and refutes those criticisms," Tabár noted in an email to AuntMinnieEurope.com. "They also selectively cite literature that supports their conclusions, neglecting a larger literature that does not."
The shortcomings of the JRSM article are threefold, according to Tabár:
- "Autier has never had access to individual breast cancer patient data of any of the Swedish trials, so he does not know which woman was or was not screened, or which case has been diagnosed in a woman who did or did not get a mammogram," he said. "The cancer registries do not provide this information. How can the authors draw conclusion about the value of screening?"
- In any analysis, the death cases from the screening epoch must be removed whose diagnosis was made before screening started. "These authors cannot do that because they do not have access to the necessary information on the individual basis, therefore, they operate with a > 50% error rate in their calculation," he said. "It is then natural that they find a lower impact of screening because they have mixed breast cancer cases from screened and unscreened women."
- "It is disconcerting that the Royal Society of Medicine has chosen to publish an article on the purported effect of mammography screening using a database lacking information on the detection and treatment modes of the individual cancer cases," he added.
Tabár urges people to retain their common sense. "We should not give poorly designed investigations and sensational, pseudoskepticism a free pass, nor any more credibility than is warranted, which in this instance, is likely to be none," he wrote.