VIENNA - Someday, assuming that today's rapid progress in biogenetics, stem cell research, and the science of tissue cultivation continue apace, there will be little need for liver transplantation. But today the supply of healthy cadaveric livers still outstrips demand by patients with end-stage liver disease, and healthy living donors are still needed to bridge the gap.
It follows that when evaluating healthy donor candidates, who are already doing their part for science and perhaps a close relative in need, MRI should be favored over CT to avoid unnecesary radiation.
But researchers from Essen, Germany, have found that CT still does a better job of defining critical vasculature, thereby enhancing overall safety for the donors. For now, they've put off plans to eliminate CT for this indication.
In a study at University Hospital Essen, Dr. Sonja Kinner, Dr. Joerg Barkhausen, and colleagues performed both preoperative CT and MR cholangiography on 20 consecutive potential living donors.
Living donor liver transplantation has become routine at University Hospital Essen, said Kinner, who presented the study Monday at the 2008 European Congress of Radiology (ECR).
"The most frequent complication, in up to 21% of the transplantations, are complications coming from the bile ducts, like stenosis, strictures, leakage, or fistulas," she said. "These complications can be prevented or minimized by clear presurgical assessment of the biliary anatomy. As these donors are mostly young and healthy patients, the purpose of our study was to compare the performance of high-resolution MR angiography and multislice CT cholangiography in the imaging of the biliary anatomy for possible variants."
The 20 candidate liver donors included 13 men and seven women (mean age 36 years). They underwent a triphasic liver CT scan that was performed on a 16-detector scanner (Sensation 16, Siemens Healthcare, Erlangen, Germany) after intravenous administration of a biliary contrast agent (Biliscopin, Bayer Schering Pharma, Berlin) at 5 mL/sec.
"We adminstered 100 mL of Biliscopin intravenously in a short infusion, 15 to 20 minutes, and 40 minutes after that we acquired the cholangiography scans," Kinner said. Only the contrast-enhanced cholangiography scans were used for the comparison.
Six to 10 days after CT the donor candidates underwent liver MRI, including MR cholangiography, on a 1.5-tesla scanner (Magnetom Avanto, Siemens) using specially adapted thin-slice half-Fourier acquisition single-shot turbo spin-echo (HASTE), T2 turbo spin-echo (TSE)* sequences, high-strength gradients, and optimized temporal and spatial resolution.
MR cholangiography was performed during a three- to five-second breath-hold, acquiring thick-slice fast T2 HASTE images in three angulations, each providing a slice thickness of 14 mm. This was followed by a triggered 3D T2 TSE* sequence, acquiring 40 2-mm-thick slices over five to seven minutes, Kinner said.
Two radiologists reviewed the images in consensus, defining variants and evaluating the visualization of the displayed biliary branches on a four-point scale, as follows:
- Only the common hepatic duct was visible.
- Right and left hepatic ducts were visible.
- Second-order branches were visible.
- Third-order hepatic branches were visible.
A statistical comparison of the results was performed using a Wilcoxon test.
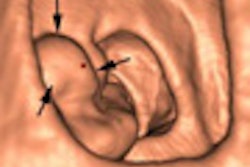
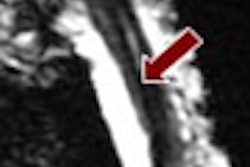
The results showed that CT cholangiography displayed significantly better delineation of the biliary tree compared to MR cholangiography (p = 0.003). The overall visualization score was 2.75 for CT versus 2.0 for MR cholangiography.
"CT mostly showed one more branch than MR cholangiography," Kinner said. "We had in three patients bile duct variants, all trifurcations."
In one patient, only the common hepatic duct could be clearly visualized on MRI, while CT visualized the biliary tree all the way to the upper confluent in the left and right hepatic duct, she noted.
As for limitations, the donor cohort was small, and "we did not analyze the arteries and veins, which are also very important for operation planning," Kinner said. "But for future directions, we think that liver-specific MR contrast agents with biliary excretion, which are now not available, might bring further improvement to show the biliary tract in MR cholangiography."
For now, contrast-enhanced CT cholangiography "is still superior," she said. "But talking to our surgeons, they say that all relevant anatomic information is now provided by MR cholangiography, so we think that MRI has potential for preoperative assessment of living donors in the future."
Session moderator Dr. Peter Huppert, director of radiology at Darmstadt Clinic in Darmstadt, Germany, questioned the need for a triphasic scan in such young patients.
The hospital scans three to four patients a week to evaluate potential donors, and nearly half have biliary tree variants, so visualizing them with contrast-enhanced CT is important for now, Kinner responded.
While the investigators had hoped to replace CT with MR following this study, which is ongoing, they have concluded that it is not yet possible. However, follow-up imaging to assess the growth of transplanted livers will be performed exclusively with MRI, Kinner said.
By Eric Barnes
AuntMinnie.com staff writer
March 10, 2008
Related Reading
At-risk liver cancer patients should get US screening, February 12, 2008
Advanced liver imaging shapes surgical strategies, September 18, 2007
Liver stiffness tied to portal hypertension in cirrhosis, May 16, 2007
Elastography noninvasively assesses hepatic fibrosis in HIV/HVC patients, February 7, 2006
Early postoperative US predicts liver transplant complications, January 6, 2006
Copyright © 2008 AuntMinnie.com