VIENNA - A new study from the U.S. and Japan found that full-laxative and minimum-laxative virtual colonoscopy (also known as CT colonography, or CTC) had equivalent sensitivities for detecting colorectal polyps 6 mm and larger, though specificity fell in the minimum-prep regimen. The patients were happy to skip the laxatives, however.
Two main types of bowel preparations are being used for VC: cathartic bowel preparation with laxatives and fecal tagging, and a "more experimental" minimum-laxative prep that relies on diet and an iodinated oral contrast agent with the addition of a fecal-tagging agent, said Janne Näppi, Ph.D., from Harvard Medical School and Massachusetts General Hospital in Boston, who presented the study led by his Harvard colleague Koichi Nagata, Ph.D. Colleagues in Tokyo and Yokohama, Japan, provided the data for the study.
The researchers aimed to prospectively compare full-laxative with minimum-laxative fecal-tagging CTC in detecting polyps with 64-detector CT, and to "specifically compare their diagnostic performance in polyp detection and assess patient acceptance," Näppi said on Friday at the 2009 European Congress of Radiology (ECR).
A total of 101 patients at elevated risk of developing colorectal cancer were evaluated, including 51 who used full-preparation CTC (1,620 mL of polyethylene glycol [PEG], followed by 400 mL of PEG-C consisting of 380 mL PEG and 20 mL sodium diatrizoate [Gastrografin]). There were 50 cases using the minimal-prep regimen (5 mL of Gastrografin after each meal for three days before scanning, plus 10 mL of a sodium picosulfate solution the night before the exam).
 |
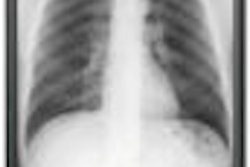
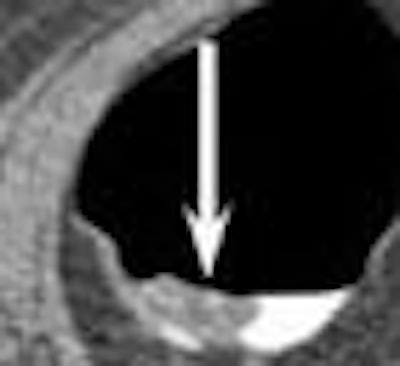
| Minimal-prep VC detected a 10-mm adenoma in the sigmoid colon (left); fecal tagging can be seen in the bright regions of the colonic lumen; colonoscopic confirmation is at right. All images courtesy of Janne Näppi, Ph.D., and Koichi Nagata, Ph.D. |
The images were acquired on a 64-detector-row CT scanner (Aquilion 64, Toshiba America Medical Systems, Tustin, CA) at 0.5-mm collimation, and automated exposure control with maximum tube current of 100-500 mAs with 120 kVp. Images were reconstructed at 0.5-mm intervals.
They were examined by two readers, both of whom were attending physicians with experience in more than 100 CTC cases. Optical colonoscopy with segmental unblinding and matching of CTC findings served as the reference standard for the study.
Just before the VC scan, patients were asked how well they had tolerated either the full-laxative or the minimum-laxative tagging-based preparation. They were asked to rate their tolerance on a scale of 1 to 5, with 1 being "well" and 5 being "poorly."
Virtual colonoscopy found 32 polyps ≥ 6 mm in the full-prep group and 23 in the minimal-prep group, most of which were adenomas and carcinomas, Näppi said.
In the full-prep with fecal-tagging subjects, per-patient sensitivity, specificity, and positive and negative predictive values for polyps ≥ 6 mm were 97%, 92%, 88%, and 98%, respectively, while those of the minimum-laxative fecal-tagging group were 88%, 68%, 56%, and 92%, respectively.
Nagata and colleagues found no statistically significant difference in sensitivities between the two methods (p > 0.05), whereas specificity was significantly lower for the minimal-prep subjects (p < 0.05). For polyps ≥ 10 mm, sensitivity was 100% in both the full-laxative fecal-tagging (15/15 polyps) and minimal-prep fecal-tagging (9/9 polyps) groups.
 |
| Results above show the numbers and histopathology of polyps ≥ 6 mm detected for full-prep (left) and minimum-prep (right) VC. Chart below shows per-patient performance for polyps ≥ 6 mm; superiority of full-laxative preparation was statistically significant in specificity but not in sensitivity. Chart at bottom depicts average per-patient performance for polyps ≥ 6 mm. Sensitivity was 100% for polyps ≥ 10 mm. |
 |
 |
The tolerance for minimal-prep VC was higher than that for the full preparation, Näppi said.
"In the minimal-preparation group, 60% of the patients tolerated the preparation well, whereas only 8% of the full-preparation group thought they tolerated the preparation well," Näppi said.
 |
| Patient tolerance was higher for the minimal-prep method. |
Full-laxative and minimum-laxative fecal-tagging CTC yielded similarly high detection sensitivities for polyps ≥ 6 mm, Näppi concluded.
"Full-laxative fecal-tagging CTC yielded a higher specificity than the minimum-laxative CTC, but the tolerance for minimal preparation was higher than for the full preparation," he said. The study is currently in press.
An informal poll of the audience suggested that many radiologists are working with minimal-prep CTC.
By Eric Barnes
AuntMinnie.com staff writer
March 7, 2009
Related Reading
ACRIN VC trial shows only small differences in bowel preps, February 9, 2009
Same-day VC prep works, but some preps are better than others, December 16, 2008
Dual-energy VC makes tagged materials disappear, October 29, 2008
Image tools cut false positives in unprepped VC, August 4, 2008
Tagging trials: Balancing image quality with patient acceptance in VC, April 16, 2008
Copyright © 2009 AuntMinnie.com