As the use of musculoskeletal ultrasound accelerates, due in part to the wider availability of handheld and portable units and the growth of image fusion, European specialists led by Dr. Andrea Klauser have developed new guidelines to inform physicians and sonographers about its appropriate clinical applications.
Evidence-based guidelines reflecting a consensus of best-practice opinion by a group of 16 experts in this specialty appear in the May issue of European Radiology. Hundreds of articles published in peer-reviewed journals were scrutinized over a two-year period to produce clinical guidelines for the six anatomical areas where musculoskeletal ultrasound is commonly employed. These include the shoulder, elbow, wrist, hip, knee and ankle/foot (Eur Radiol, 2012, Vol. 22:5, pp. 1140-1148).
 Side-by-side fusion imaging of real-time high-frequency ultrasound and MR images show the pediatric spine in a neonate with meningitis. Image courtesy of GE Healthcare.
Side-by-side fusion imaging of real-time high-frequency ultrasound and MR images show the pediatric spine in a neonate with meningitis. Image courtesy of GE Healthcare.Concerned that ordering musculoskeletal ultrasonography is often based on the experience of a referring physician or sonographer, the European Society of Musculoskeletal Radiology (ESSR) selected a panel of experts from Austria, Belgium, Denmark, France, Italy, the Netherlands, and the U.K. in 2008 to work on the guidelines. Recommendations were based on the clinical condition, its level of evidence, the strength of the recommendations, and the percentage of agreement. Each clinical indication was then given an appropriateness grade, from zero (ultrasound not indicated) to three (ultrasound = first exam choice).
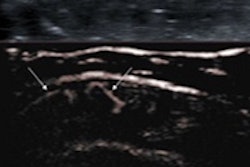
Musculoskeletal ultrasound exams should be ordered to detect joint synovitis, fluid, and septic effusion for potential aspiration. It is relevant to image most joints, but it is poor at detecting loose bodies, the authors noted.
Specifically, the group identified 31 types of clinical indications for wrist imaging, of which 16 received the highest appropriateness rating. Ultrasound is not indicated for hamate fractures, triangular fibrocartilage complexes, capitate fractures, Kienböck's disease, or hamatolunate impingements, they noted.
Twenty-one clinical indications were identified for the elbow. Eleven ranked as a "first exam choice." It was not recommended for lateral collateral ligament, supracondylar elbow fracture and postoperative positioning, or for lateral condyle fractures in pediatric patients.
 Lead author Dr. Andrea Klauser from Innsbruck.
Lead author Dr. Andrea Klauser from Innsbruck.
The shoulder was assigned 23 clinical indications of which only six received a "first exam choice" rating. Musculoskeletal ultrasound is not indicated for adhesive capsulitis, gelenohumeral joint traumatic and dynamic instability, or Parsonage-Turner syndrome.
The ankle and foot had 27 clinical indications identified, with more than half (15) receiving a top rating. The exam was not indicated for posterior talo-fibular ligaments, intra-articular diseases, cartilage lesions, and fractures of either the distal tibulous or talus.
For the knee, 29 clinical indications were identified, of which only 10 were top rated. Ultrasound is not recommended for posterolateral corner lesions, intra-articular ganglion, or Hoffa's fat pad syndrome.
Twenty-one indications were identified for the hop, with six receiving top rating for a musculoskeletal ultrasound exam. It should not be ordered to image an intra-articular snapping hip, osteoarthritis, low-grade muscle injuries, growing pain, sciatica, psoas tendon problems, or trochanteric pain.
Lead author Dr. Andrea Klauser, a radiologist at the Medical University Innsbruck in Austria, and colleagues have developed an easy to read table for each anatomic area, plus an additional table summarizing all the clinical indications where the examination is recommended.
The authors said further high-quality research is needed, but they also said their work provides a useful tool for the rational use of musculoskeletal ultrasound regardless of the clinician's experience examining a patient with this imaging modality.