Digital workflows using open-source software and desktop 3D printing can be a practical and cost-effective solution for patient-specific preoperative planning for advanced endovascular repair in centers without access to costly commercial planning platforms or custom devices.
In a report published on 26 November in Cureus, Dr. Juan Carlos Gomez-Rodriguez of the Vascular Surgery Department at Clinica Medellin, Colombia, described a reproducible digital workflow for a physician-modified endograft for an endovascular aortic aneurysm repair (EVAR) of a complex abdominal aortic aneurysm (AAA).
Using this workflow, a 78-year-old man with an infrarenal AAA and a prior failed EVAR underwent successful reintervention, the authors wrote.
 Postoperative CT angiography at presentation shows type Ia and type IIIa endoleaks. (A) Multiplanar reconstruction in a predominantly sagittal plane with maximum intensity projection (MIP) showing a type IIIA endoleak (black arrow) caused by disconnection between the limb extension and the branch of the Anaconda bifurcated endograft. (B) Multiplanar reconstruction in a mainly coronal plane with MIP demonstrating a type 1A endoleak (blue arrow) originating from the proximal seal zone and extending into the aneurysmal sac.Dr. Juan Carlos Gomez-Rodriguez et al and Cureus
Postoperative CT angiography at presentation shows type Ia and type IIIa endoleaks. (A) Multiplanar reconstruction in a predominantly sagittal plane with maximum intensity projection (MIP) showing a type IIIA endoleak (black arrow) caused by disconnection between the limb extension and the branch of the Anaconda bifurcated endograft. (B) Multiplanar reconstruction in a mainly coronal plane with MIP demonstrating a type 1A endoleak (blue arrow) originating from the proximal seal zone and extending into the aneurysmal sac.Dr. Juan Carlos Gomez-Rodriguez et al and Cureus
The workflow uses open-source imaging software for centerline extraction, anatomical segmentation, and stereolithography (STL) model creation, and AI-assisted scripting to generate cylindrical fenestrated templates.
The Medellin team wrote that while physician-modified endografts (PMEGs) have increasingly proven to be a practical alternative to costly custom-made fenestrated devices, especially for urgent or anatomically complex cases, a successful outcome is dependent on thorough preoperative planning, precise fenestration alignment, and intraoperative accuracy.
The use of digital tools and templates can reduce variability, increase reproducibility, and therefore increase the likelihood of success, according to the authors. Furthermore, the incorporation of AI to automate processes such as generating the cylindrical template used to guide fenestration in the procedure further improves the reproducibility of the workflow.
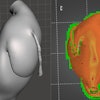
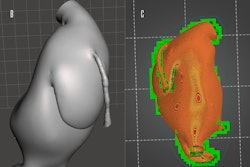
Along with the template, the workflow also created a patient-specific anatomical reconstruction, generated in 3D Slicer, which served to provide spatial orientation, while the template served as what the authors referred to as “a quick intraoperative stencil for PMEG modification.”
 Postoperative 3D volume rendering of the fenestrated endograft reconstruction: 3D volume-rendered reconstruction obtained in Horos using the standard soft-tissue preset. The image displays the postoperative appearance of the fenestrated endograft and visceral stents, extending from the descending thoracic aorta to the iliac bifurcation, acquired during the follow-up CT angiogram one month after the procedure. The reconstruction shows patent visceral branches with well-perfused stents, absence of endoleak, and successful restoration of the previously disconnected left limb with adequate iliac perfusion.Dr. Juan Carlos Gomez-Rodriguez et al and Cureus
Postoperative 3D volume rendering of the fenestrated endograft reconstruction: 3D volume-rendered reconstruction obtained in Horos using the standard soft-tissue preset. The image displays the postoperative appearance of the fenestrated endograft and visceral stents, extending from the descending thoracic aorta to the iliac bifurcation, acquired during the follow-up CT angiogram one month after the procedure. The reconstruction shows patent visceral branches with well-perfused stents, absence of endoleak, and successful restoration of the previously disconnected left limb with adequate iliac perfusion.Dr. Juan Carlos Gomez-Rodriguez et al and Cureus
The cylindrical template took under two hours to print; it was sterilized with low-temperature plasma before use, the team noted. During the procedure, the sterile 3D-printed cylindrical stencil was positioned over the surface of the endograft fabric, and each planned fenestration was marked through the corresponding openings of the stencil to delineate the exact locations for the visceral vessels to ensure correct alignment with the preoperative plan.
Following the type IIIa endoleak repair and confirmation that it was fully corrected, the patient’s postoperative course was uneventful, and he was discharged three days postprocedure in stable condition, the researchers reported.
“A follow-up CTA obtained one month later confirmed complete exclusion of the aneurysm, absence of endoleaks, and patent visceral branches with preserved perfusion,” they wrote.
Not only does this case demonstrate the utility of 3D printing in aortic repair but also the utility of AI-assisted modeling in creating guides for PMEG planning, improving workflow through precision and reproducibility, the team concluded.
To facilitate the adoption of their workflow, the authors share in the article the AI-assisted Blender script they used in the procedure.
The full report may be read on the Cureus website.