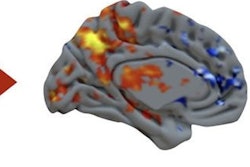
Acute penile pathologies are rare in the emergency department, but both radiologists and clinicians must be able to recognize the most frequent and severe acute conditions and be aware of the treatments, Spanish researchers have emphasized.
Ultrasound is the technique of choice in penile emergencies. The modality can be used to evaluate the anatomical and physiological integrity of the penis and to assess its vascularity using color Doppler, noted Dr. Iñigo Zubiaguirre Telleria and colleagues from the Hospital Universitario Severo Ochoa, Leganés, Madrid.
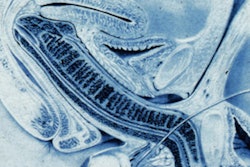
 Superficial dorsal vein thrombosis. Color Doppler in transverse (A) and longitudinal (B) planes. The images show an absence of signal from the superficial dorsal vein of the penis and echogenic material related to thrombus (arrow). Presence of flow in the cavernous artery (arrowhead). All figures courtesy of Dr. Iñigo Zubiaguirre Telleria et al and European Society of Radiology (ESR) EPOS database.
Superficial dorsal vein thrombosis. Color Doppler in transverse (A) and longitudinal (B) planes. The images show an absence of signal from the superficial dorsal vein of the penis and echogenic material related to thrombus (arrow). Presence of flow in the cavernous artery (arrowhead). All figures courtesy of Dr. Iñigo Zubiaguirre Telleria et al and European Society of Radiology (ESR) EPOS database.
The penis comprises three erectile structures: a pair of corpora cavernosa, located along the dorsolateral aspect of the penis; and the corpus spongiosum, which lies in the midline and on the ventral surface of this organ (it contains the penile urethra). These structures are individually covered by the tunica albuginea, they explained.
The study must be done with high-frequency linear probes (around 10-18 mHz), and it's vital to apply B-mode ultrasound imaging to assess morphological data and to use color and spectral Doppler techniques for the evaluation of arterial and venous flow. Develop a routine protocol to carry out a correct exam, they continued.
"The penis should be examined from both its dorsal and ventral surface, and it should be observed in a transverse and longitudinal plane," the authors pointed out. "The patient should be lying on the medical examination table in the supine position, with his legs extended and close together to contain the external genitalia. A considerable amount of ultrasound gel should be used to produce a high-quality image without acoustic interruption."
Ultrasound is useful in delimiting the hematoma, knowing its exact measurements and its relationship with the tunica albuginea, which indicate the therapeutic decision. These diseases can occur both with the penis at rest or during erection, but when it is erect, there is a greater risk of rupture of the tunica albuginea, they pointed out.
 Penile fracture. B-mode ultrasound in the transverse (A) and longitudinal (B) planes. A large extratunical hematoma can be seen adjacent to the erectile bodies of the penis (star). In the longitudinal plane, a loss of continuity of the tunica albuginea (arrow) confirms its rupture.
Penile fracture. B-mode ultrasound in the transverse (A) and longitudinal (B) planes. A large extratunical hematoma can be seen adjacent to the erectile bodies of the penis (star). In the longitudinal plane, a loss of continuity of the tunica albuginea (arrow) confirms its rupture.
Penile fracture is caused by a traumatic rupture of the tunica albuginea, and it occurs due to a sudden flexion of the erect penis during sexual intercourse or masturbation. Patients report hearing a cracking sound followed by sudden pain and detumescence, swelling, and deformity of the penis. It is associated with urethral injury in 10% to 20% of cases, and the treatment is always surgical, according to Telleria and colleagues. Ultrasound is the imaging test of choice to confirm the diagnosis.
Ultrasound findings include loss of continuity of the hyperechoic line of the tunica albuginea, presence of hematoma adjacent to the area of rupture, and indirect signs of urethral injury, such as air inside the corpora cavernosa. If ultrasound is inconclusive, retrograde urethrography should be performed.
 Abscess. B-mode ultrasound image (A) shows a heterogeneous collection with a central hypoechoic area and detritus inside the lesion (star). Color Doppler (B) shows an increased vascularity in the peripheral soft tissues (arrow).
Abscess. B-mode ultrasound image (A) shows a heterogeneous collection with a central hypoechoic area and detritus inside the lesion (star). Color Doppler (B) shows an increased vascularity in the peripheral soft tissues (arrow).
A penile abscess typically requires therapeutic drainage. On ultrasound, it's visualized as a hypoechoic collection with debris and/or internal septa, without a Doppler signal inside the lesion. In some cases, it may contain gas bubbles, they added.
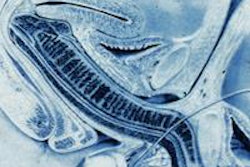
Priapism occurs when a pathological penile erection persists for four hours or more and is not related to sexual stimulation. It is classified as low-flow priapism (ischemic or veno-occlusive) and high-flow priapism (not ischemic or arterial). Imaging tests are not usually necessary, and cavernous blood gas levels can help to confirm the diagnosis, the Madrid team stated.
 Nonischemic or high-flow priapism. Color Doppler in the transverse plane (A) and spectral Doppler in the longitudinal plane (B). Turbulent flow of the left cavernous artery is observed (arrow). The lesion shows a low resistance pattern, with increased systolic and diastolic velocities. These findings are related to a penile pseudoaneurysm.
Nonischemic or high-flow priapism. Color Doppler in the transverse plane (A) and spectral Doppler in the longitudinal plane (B). Turbulent flow of the left cavernous artery is observed (arrow). The lesion shows a low resistance pattern, with increased systolic and diastolic velocities. These findings are related to a penile pseudoaneurysm.
Superficial dorsal vein thrombosis, or penile Mondor disease, is a benign and self-limiting process that affects sexually active men, especially during penile erection. It requires a clinical diagnosis (indurated cord on the dorsal aspect of the penis), but ultrasound helps to confirm the diagnosis and enables a follow-up to exclude a possible underlying tumor.
The treatment is conservative -- i.e., sexual rest and nonsteroidal anti-inflammatory medications -- and anticoagulation is not necessary, they noted.
Ultrasound findings include absence of flow and compressibility of the superficial dorsal vein of the penis. "It is possible to identify echogenic material within the vein that confirms the thrombus. In some cases, an increase in the caliber of the vein and inflammation of the adjacent soft tissues are observed," Telleria and colleagues stated.
You can read the full e-poster on the EPOS database of the ESR. The work was presented at ECR 2024. The coauthors were Drs. A. De Miguel Alvarez-Vieitez, J.H. Álvarez Cuenca, J.M. Sánchez Bermejo, I. Vidal, Á. Cindonga Rodríguez, A.N. Ani, W.A. Ocampo Toro, and M.A. Hoyas Garcia.