Imaging of facial fractures is challenging, but the optimal use of CT scan can provide a path to diagnosis in polytraumatic and unconscious patients, as well as in cases of severe soft tissue lesions, according to award-winning research.
“Certain clinically and/or surgically relevant structures should be borne in mind and assessed,” Dr. Mónica Régil Guerrero and colleagues at the Hospital Universitario Donostia in San Sebastián, Spain, noted in an e-poster that received a magna cum laude award at ECR 2025. “Multiplanar and volume-rendered reconstructions must be systematically revised.”
 Bilateral frontal fracture involving both the anterior and posterior wall of both frontal sinuses (3D and red arrows). The fracture spreads inferiorly to both superior orbital rims (magenta arrows), posteriorly towards the anterior cranial fossa, with a resulting pneumocephalus bubble (blue arrow), and medially (yellow arrow in the axial view). Nevertheless, both frontonasal ducts remain intact (yellow arrows in sagittal views). AX = axial view, COR = coronal view, SAG = sagittal view, 3D = volume-rendered reconstruction. All figures courtesy of Dr. Mónica Régil Guerrero et al and presented at ECR 2025.
Bilateral frontal fracture involving both the anterior and posterior wall of both frontal sinuses (3D and red arrows). The fracture spreads inferiorly to both superior orbital rims (magenta arrows), posteriorly towards the anterior cranial fossa, with a resulting pneumocephalus bubble (blue arrow), and medially (yellow arrow in the axial view). Nevertheless, both frontonasal ducts remain intact (yellow arrows in sagittal views). AX = axial view, COR = coronal view, SAG = sagittal view, 3D = volume-rendered reconstruction. All figures courtesy of Dr. Mónica Régil Guerrero et al and presented at ECR 2025.
Facial trauma often presents itself in a high-energy polytraumatic context, with severe soft tissue lesions that limit physical examination of the bony structures underneath, thus making the diagnosis almost entirely dependent on an emergency CT scan, they explained. Facial fractures tend to be complex and difficult to assess, classify, and report for radiologists. Delivering an optimal report requires a basic knowledge of facial anatomy, fracture types, and surrounding structures that may be affected.
The CT scan images should be acquired in a parallel plane to the hard palate and include every structure located between the frontal sinuses and the mandibular symphysis. Two sets of images should be acquired: bony-window axial images, no more than 1 mm thick, allowing for optimal sagittal and coronal multiplanar reconstructions; and thicker, soft tissue-window axial images that are appropriate for volume-rendered reconstructions. No intravenous contrast is required unless a vascular lesion is suspected, the researchers pointed out.
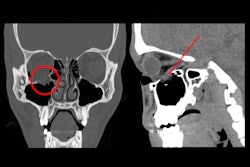
 The images on the left side of the white vertical bar show a bilateral, simple, and nondisplaced nasal fracture. The nasofrontal suture (orange arrows), nasal septum (green arrow), and anterior nasal spine (yellow circles) remain intact, while the fracture line crosses the left nasomaxillary suture (red arrows). On the other hand, the image on the right contains a bilateral, comminuted, and displaced nasoseptal fracture (red circle), in which the nasal septum is also involved (red arrow).
The images on the left side of the white vertical bar show a bilateral, simple, and nondisplaced nasal fracture. The nasofrontal suture (orange arrows), nasal septum (green arrow), and anterior nasal spine (yellow circles) remain intact, while the fracture line crosses the left nasomaxillary suture (red arrows). On the other hand, the image on the right contains a bilateral, comminuted, and displaced nasoseptal fracture (red circle), in which the nasal septum is also involved (red arrow).
In facial fractures, the standard aspects to be reported are the unilateral or bilateral involvement of bones, as well as the presence of comminution or displacement.
“The most commonly fractured structure in the frontal bone is the anterior wall of the frontal sinus, followed by both the anterior and posterior walls,” they stated. “Whenever the posterior wall alone is fractured, the skull base and cranial vault should be examined, as they could harbor the source fracture.”
Frontal fractures can occur in three ways:
- Inferiorly: The superior orbital rim will be involved.
- Medially: The frontonasal duct should be checked because this is the drainage tract of the frontal sinus into the nasal cavity, through the middle nasal meatus; when this is fractured, a mucocele can arise.
- Posteriorly: The anterior cranial fossa is immediately behind the frontal bone; therefore, cerebrospinal fluid leak, encephalocele, pneumocephalus, and traumatic or infectious intracranial complications may occur.
 Pure and simple blow-out left orbital fracture; the orbital rim and internal orbital buttress remain unaltered. Over half of the orbital floor is involved (measurement in the lower left image), and the fracture line crosses the infraorbital canal (yellow circle). The left inferior rectus muscle (yellow arrow) looks asymmetrical when compared to the contralateral one and appears to be “tractioned” with accompanying intraorbital fibrofatty tissue into the left maxillary sinus (dark green arrow); the sinus also has hyperdense content compatible with a hematoma (red arrow).
Pure and simple blow-out left orbital fracture; the orbital rim and internal orbital buttress remain unaltered. Over half of the orbital floor is involved (measurement in the lower left image), and the fracture line crosses the infraorbital canal (yellow circle). The left inferior rectus muscle (yellow arrow) looks asymmetrical when compared to the contralateral one and appears to be “tractioned” with accompanying intraorbital fibrofatty tissue into the left maxillary sinus (dark green arrow); the sinus also has hyperdense content compatible with a hematoma (red arrow).
The most common fractures are blow-out fractures involving the orbital floor or, less frequently, the medial wall. Acute inflammation and hemorrhage could either mask enophthalmos due to an orbital blow-out fracture or lead to an orbital compartment syndrome; both these conditions require surgical intervention, the authors noted.
Le Fort fractures are three specific patterns of midface fracture, whose compulsory common factor is the involvement of the pterygoid plates. Le Fort fractures can be either isolated or simultaneous, unilateral or bilateral, symmetric or asymmetric, and complete (separate fragments) or incomplete (greenstick fractures).
Due to its shape, the mandibular bone will often develop two different fractures: a primary one at the area of direct trauma and a secondary contralateral one due to force transmission, the researchers noted. The condition of the mandibular canal, the presence of basal triangles, and dentoalveolar fractures should be reported because surgery may be necessary, they added.
 The images on the left side of the vertical white bar show a bilateral mandibular fracture. The left fracture (light yellowish-brown arrows) is located in the mandibular angle and crosses the mandibular canal, causing a fragment displacement of more than 5 mm (measurement in lower right image). The nondisplaced right fracture (orange arrows) is subtle in the parasymphyseal region, but it appears to involve the mental foramen. The images on the right side of the vertical white bar illustrate a bifocal left mandibular fracture. A comminuted and displaced (lower right image) fracture involves the symphyseal and parasymphyseal regions (orange arrows) and the mandibular body (lavender arrows) and crosses the mental foramen of the mandibular canal. The other fracture is a subcondylar luxation fracture (light blue arrows) with >35º angled fragments (light blue angle).
The images on the left side of the vertical white bar show a bilateral mandibular fracture. The left fracture (light yellowish-brown arrows) is located in the mandibular angle and crosses the mandibular canal, causing a fragment displacement of more than 5 mm (measurement in lower right image). The nondisplaced right fracture (orange arrows) is subtle in the parasymphyseal region, but it appears to involve the mental foramen. The images on the right side of the vertical white bar illustrate a bifocal left mandibular fracture. A comminuted and displaced (lower right image) fracture involves the symphyseal and parasymphyseal regions (orange arrows) and the mandibular body (lavender arrows) and crosses the mental foramen of the mandibular canal. The other fracture is a subcondylar luxation fracture (light blue arrows) with >35º angled fragments (light blue angle).
“As for further studies, I have not considered nor thought about anything specific yet, but I am definitely open to suggestions,” Guerrero, who is at the end of her second year of radiology residency, told AuntMinnieEurope.com on 10 April.
You can read the full ECR 2025 poster here. The co-authors of this exhibit were Ainhoa Goikoetxea Zubeldia, Mikel Irizar Dorronsoro, Maria Queralt Caballero Lladó, Ainara Aramburu, Irati Elizasu Roteta, Oihane Iñarra, Paula Gabriela Aguinagalde Vives, and Marina Isabel Blanco.