The diagnosis of infective endocarditis remains a serious clinical challenge, but F-18 FDG PET/CT is making progress and can be an extremely useful modality in these patients, with good sensitivity and specificity, three different research groups from Portugal, France, and Italy reported at the recent European Society of Cardiology (ESC) virtual congress.
Improvements have occurred in the management of infective endocarditis, but it is still a deadly disease. Echocardiography is vital for diagnosis, but it is operator-dependent, and its sensitivity can fall in the presence of valvular prosthesis.
Molecular imaging's role is growing in this area, as was evident from the findings of three studies presented at ESC 2020.
Pearls from Portugal
PET/CT is of value in suspected cases of both native valve endocarditis (NVE) and prosthetic valve endocarditis (PVE), according to Dr. Jose Paulo Lopes De Almeida at the University Hospitals of Coimbra, Portugal.
"It allowed the identification of the cause of clinical scenario in more than 50% of patients in which the diagnosis was excluded," noted De Almeida, adding that the use of F-18 FDG PET/CT has resulted in a significant decrease in the number of potential cases of endocarditis at his facility.
The diagnostic accuracy of the modified Duke Criteria for diagnosing endocarditis is suboptimal, especially in the presence of PVE, he explained.
The Coimbra team evaluated 82 patients (62% men, mean age of 61 ± 19 years) referred for F-18 FDG PET/CT between May 2016 and June 2019. De Almeida and colleagues assessed the final diagnosis given for each patient by the endocarditis group at the time of discharge or death, after seeing the clinical, microbiological, and imaging information as well as the clinical response to treatment.
The researchers found 67 PET/CT results concordant with the final diagnosis, corresponding to a 96% agreement (k = 0.91, p = 0.04). A maximum standardized uptake value (SUVmax) cutoff value of ≥ 3.1 identified positive cases with 88.9% sensitivity and 70% specificity.
"In patients with NVE, the addition of PET/CT to the [mean distance to conformity] resulted in a reduction of the number of possible infective endocarditis cases from 58% to 4.3%," they stated. "In patients with PVE/intracardiac devices, PET/CT allowed reclassification of 67.4% of possible cases to 4.2%. An alternative diagnosis was provided in 55.6% of the negative infective endocarditis cases."
Musings from Marseille
The usefulness of F-18 FDG PET/CT is high for embolic detection, asserted cardiologists Dr. Mary Philip and Dr. Gilbert Habib and colleagues from the Hospital La Timone of Marseille, France, in another ESC 2020 presentation on endocarditis. Also, diffuse splenic uptake represents a possible new diagnostic criterion for NVE, they reported.
F-18 FDG PET/CT was added to the ESC guidelines for infective endocarditis in 2015 and the modality is currently recommended for patients with suspected prosthetic valve and cardiac device infective endocarditis. However, the value of the ESC classification is unknown in patients with NVE, and uncertainty often surrounds the clinical impact of PET/CT findings, they elaborated.
The Marseille group's prospective study included 75 patients with suspected NVE who underwent F-18 FDG PET/CT between 2012 and 2017. The team excluded patients with uninterpretable or infeasible PET/CT scans. Using gold-standard expert consensus, 63 cases of infective endocarditis were confirmed and 12 were rejected.
Philip and Habib observed significant valvular uptake in 11 of the 63 patients, and no patients with rejected infective endocarditis (18% sensitivity, 100% specificity). A peripheral embolism or mycotic aneurysm was seen in 20 cases (32%).
"Application of ESC criteria increased the sensitivity from 64% to 70% (p < 0.001) without any change in specificity," they pointed out. "A [diffuse splenic uptake] was observed in 39 (52%) patients, including 37 patients with a final diagnosis of NVE (specificity 83%)."
Insight from Italy
Italian investigators also confirmed the valuable diagnostic role of F-18 FDG PET/CT, as well as its importance for identifying septic embolic sites or alternative causes of infection/inflammation.
Dr. Roberto Boni, a nuclear medicine specialist at the Papa Giovanni XXIII Hospital in Bergamo, and colleagues evaluated 90 patients (60 men and 30 women; mean age, 67 ± 16 years; median age, 72; range 18-88) who underwent F-18 FDG PET/CT between January 2015 and January 2019 to define which pattern of uptake and semiquantitative parameters (SUVmax, valve/liver, valve/lung, and valve/mediastinum uptake ratio) present the highest diagnostic accuracy for infective endocarditis. They excluded patients with permanent cardiac devices.
Overall, PET/CT achieved a sensitivity rate of 96% and a specificity rate of 75%. A focal pattern of uptake was found in 17 out of 30 confirmed cases of infective endocarditis (mean SUVmax = 5.29 ± 1.8, median SUVmax = 5.5), whereas a diffuse pattern of uptake was found in 11 confirmed cases of infective endocarditis (mean SUVmax = 8.1 ± 3.5, median SUVmax = 7.6). No significant differences were found between the valve/liver and the valve/mediastinum uptake ratios of positive and negative patients with either focal or diffuse pattern of uptake.
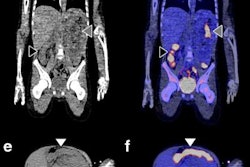
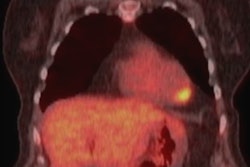
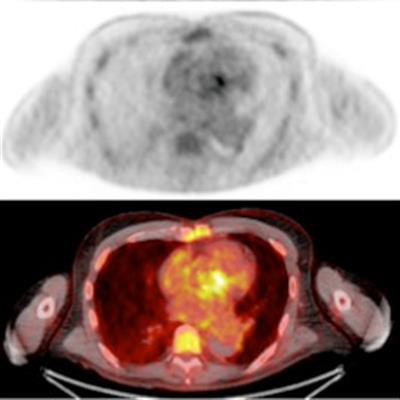
 F-18 FDG PET/CT in a 59-year-old male patient with aortic valve infective endocarditis caused by Escherichia coli. He had fever and diffuse articular pain. He was previously diagnosed with ascending aorta aneurism, aneurism of the Circle of Willis, thoracoabdominal aortic aneurysm, and finally type A aortic dissection. History of aortic valve prosthesis infectious endocarditis (Staphylococcus epidermidis) treated with antimicrobial therapy. PET/CT images confirm infectious endocarditis, showing F-18 FDG uptake at the aortic valve infective prosthesis (A, from top to bottom nonattenuated PET, attenuated PET, and fused PET/CT). Additionally, F-18 FDG PET/CT shows aortic arch graft infection involving mediastinal soft tissues and the sternum (B and C, attenuated PET and fused PET/CT). Images courtesy of Dr. Martina Sollini, Humanitas University, Italy.
F-18 FDG PET/CT in a 59-year-old male patient with aortic valve infective endocarditis caused by Escherichia coli. He had fever and diffuse articular pain. He was previously diagnosed with ascending aorta aneurism, aneurism of the Circle of Willis, thoracoabdominal aortic aneurysm, and finally type A aortic dissection. History of aortic valve prosthesis infectious endocarditis (Staphylococcus epidermidis) treated with antimicrobial therapy. PET/CT images confirm infectious endocarditis, showing F-18 FDG uptake at the aortic valve infective prosthesis (A, from top to bottom nonattenuated PET, attenuated PET, and fused PET/CT). Additionally, F-18 FDG PET/CT shows aortic arch graft infection involving mediastinal soft tissues and the sternum (B and C, attenuated PET and fused PET/CT). Images courtesy of Dr. Martina Sollini, Humanitas University, Italy."Interestingly, in the presence of diffuse valve uptake, both SUVmax and the valve/lung ratio were significantly higher in patients with a final diagnosis of infective endocarditis, including the group of patients under antimicrobial treatment (> 90%)," Boni and colleagues observed. "PET/CT confirmed its ability to identify extracardiac sites of F-18 FDG PET/CT uptake in the presence of septic embolism (35%) and in patients with other diseases such as vasculitis, vascular prosthesis infections, mediastinitis, and cancer, particularly in patients with infective endocarditis sustained by Streptococcus gallolyticus."
However, nuclear cardiac imaging analysis may be tricky, and methodological and technical aspects must be carefully considered, they concluded.