Mobile stroke ambulances equipped with a CT scanner and medical personnel can greatly improve the accuracy and efficiency of determining which stroke patients require surgical treatment, compared with standard clinical decision-making, according to a study published online on 3 September in JAMA Neurology.
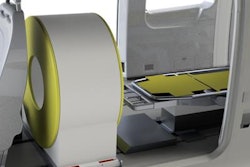
In recent years, several healthcare systems have been providing stroke care directly at the site of patient injury by sending out an ambulance equipped with a CT scanner, a point-of-care laboratory, telecommunication capabilities, and a team of emergency clinicians that includes a paramedic, stroke physician, and a radiologist. The mobile stroke unit intervention generally consists of a neurologic exam, point-of-care tests, and a CT scan.
Multiple studies conducted in Europe and the U.S. have shown that mobile CT stroke units have helped reduce treatment times for patients requiring clot-busting medication.
Yet few, if any, studies have investigated the potential of these mobile units to help resolve a major issue in stroke management: delayed surgical treatment for patients found to have a clot at a primary stroke center who then need to be transferred to a separate comprehensive center capable of performing thrombectomy, according to lead author Stefan Helwig from Saarland University Hospital and colleagues from Germany.
Thus, the researchers set out to assess the effectiveness of mobile CT units at distinguishing between stroke patients who required interventional treatment and those who could safely be managed at a primary stroke center. They specifically examined a mobile CT unit that serviced individuals in the German state of Saarland and compared it with the standard operating procedure of using the Los Angeles Motor Scale (LAMS) stroke severity scale.
The researchers evaluated the cases of 116 stroke patients whose prehospital management followed either the standard clinical criteria method or the route of mobile stroke care. Patient surveillance lasted for three months following initial presentation at some point between June 15, 2015, and November 15, 2017.
Overall, clinicians using mobile stroke care made an accurate triage decision for all the patients, compared with roughly 70% when using the standard approach.
In addition to more efficient triage, the researchers found that mobile stroke units significantly improved various metrics of stroke management, including the amount of time that elapsed between the stroke and when the patient first started receiving medical attention, underwent a CT or MRI exam, and received clot-busting therapy.
| Prehospital stroke management with mobile CT unit vs. standard of care | ||
| Standard clinical scoring criteria | Mobile CT | |
| % of patients sent to appropriate treatment center | 69.8% | 100% |
| % of patients requiring secondary transfer | 41.2% | 0% |
| Time until 1st contact for stroke care | 41.5 min | 10.3 min |
| Time until end of imaging exam | 80 min | 39.3 min |
The benefits afforded by mobile CT did not lead to statistically significant differences in long-term patient outcomes, although the study was not powered to determine significance in this aspect of care, the authors noted.
These findings do not negate the value of relying on clinical decision-making in acute stroke care, but rather they establish a foundation of evidence for a viable alternative with benefits of its own, wrote Drs. Jason McMullan and Pooja Khatri, from the University of Cincinnati in the U.S., in an accompanying editorial.
"Even if mobile stroke units are consistently 100% accurate, worldwide integration of mobile stroke units into stroke systems of care is not feasible; there will always be a role for clinical decision-making, and such clinical judgment will always be imperfect," they concluded. "We must define our priorities for prehospital stroke identification and triage and agree on what is 'good enough.' "