At higher field strengths, the hope is for new technology to lead to more clinical applications benefiting from homogeneous MR images, but can it ever be cost-effective? That was the main question addressed during a round table discussion at the recent meeting of the European Society of MR in Medicine and Biology (ESMRMB) in Toulouse, France.
At the session, experts outlined the promise of parallel transmit (pTX) whole-body MRI and how it is already improving abdominal and prostate cancer detection and changing individual patient outcomes. The next couple of years will be a learning curve in understanding how independent pTX channels can improve image quality and change patient or even MR management, and future clinical systems could include eight, 16, or even 32 channels at field strengths of up to 7 tesla, they believe.
"We are only at the beginning of the journey," said Dr. Stefan Haneder, the section chief of vascular and abdominal imaging at the Institute of Clinical Radiology and Nuclear Medicine at University Medical Center Mannheim in Germany and a panel speaker during a discussion focusing primarily on the cost benefits of pTX whole-body MRI.
 Multitransmit whole-body MRI will save more lives, according to Dr. Stefan Haneder.
Multitransmit whole-body MRI will save more lives, according to Dr. Stefan Haneder.
Although pTX is not yet widely used, it improves patient outcomes, according to Haneder. "My view is that pTX is worth the money. I'm convinced the extra money spent will contribute to saving lives," he said. "Everyone should invest in this if they want to use 3T in clinical practice."
At field strengths above 1.5 tesla, the central parts of the abdomen, such as the pancreas, are often inhomogeneous due to standing wave artifacts. This is because at 3 tesla and above, the wave length is normally shorter than the human abdomen. These artifacts can be largely overcome by pTX improving the homogeneity of the B1 field, enabling more quantitative MRI and dramatically impacting patient management.
"After the wide implementation of parallel imaging on the receive side in our daily practice, which has increased the speed of multiple MR protocols, pTX will bring the next boost for MRI on the transmit side," Haneder told AuntMinnieEurope.com, outlining how the technique is already routinely implemented in his department on a 3-tesla system with two independent transmit channels, as opposed to the earlier systems with two dependent channels.
This latest generation of pTX allows improvements such as modified sequences that reach far beyond B1 shimming, he explained. On new machines, specialists can use the two transmit channels independently in terms of amplitude, phase, and dynamic radiofrequency (RF) wave forms for arbitrary shaped excitation, whereas MR units equipped with two dependent transmit channels only allow different amplitudes or phases.
"Now we can create pulse schemes as desired, to excite parts of the body, single organs, or vessels, for example. Furthermore, we can excite a smaller field-of-view if needed and truly increase spatial resolution," Haneder said.
One of the modified sequences that benefits from two independent transmit channels is known as the zoomed technique, which reduces the field-of-view to save phase-encoding steps and thus imaging time. It is already routinely implemented for the abdomen in Mannheim in combination with diffusion-weighted imaging (DWI) based on single-shot, spin-echo echo-planar imaging (EPI). With zoomed EPI-DWI, it is possible to reduce the field-of-view without ghosting artifacts and with vastly reduced distortion artifacts.
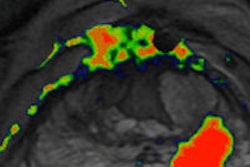
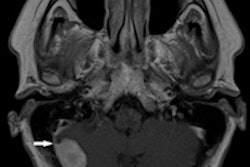
 Zoomed EPI-DWI using pTX MRI can allow clearer visualization of transitional cell carcinoma and renal abscess. Images courtesy of Dr. Stefan Haneder.
Zoomed EPI-DWI using pTX MRI can allow clearer visualization of transitional cell carcinoma and renal abscess. Images courtesy of Dr. Stefan Haneder.
"In the pancreas, intraductal papillary mucinous neoplasms (IPMNs) can be visualized as small cystic lesions. One criterion for the likelihood of malignancy is the presence of intramural nodules. With zoomed EPI-DWI, visualization and even ADC value assessment of small lesions within the cysts is possible," he said.
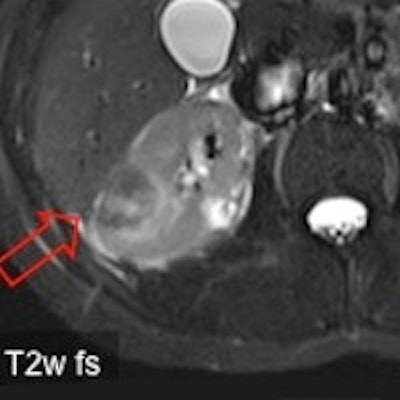
Other anatomical regions where this zoomed technique can lead to a clinical improvement include head and neck applications, other abdominal organs such as the kidneys, and also in the prostate, according to Haneder. If a biopsy is negative, despite high prostate-specific antigen (PSA) values and suspected prostate cancer, a multiparametric MR, including T2-weighted morphology, DWI, perfusion, and spectroscopy, is one route for detecting prostate cancer and guiding a further needle biopsy.
"Artifacts such as geometric distortion often hamper DWI of the prostate. In many cases, this can be solved by zoomed EPI-DWI for higher quality visualization; reduced geometric distortions allow an accurate fusion of functional DWI and morphology," he stated. "From a clinical point of view, this technique could and should become routine as a perfect MR detection tool for patients with high PSA values but negative biopsies."
Zero tolerance on artifacts
Co-speaker Jo Hajnal, PhD, said there is now no place for accepting artifacts at high field strengths when it comes to scanner design.
"Continuing to operate on the basis that the RF fields are uniform is yesterday's story and doesn't work very well with today's higher magnet strengths," said Hajnal, a professor of imaging sciences in the department of biomedical engineering and a member of the Centre for the Developing Brain at King's College London.
The transmitting RF coils used in most current clinical MR systems derive from designs developed when lower field magnets were the norm, he explained. At higher magnetic fields, such as 3 tesla and beyond, the presence of the subject in the system has an impact on the performance of the transmit coil, so that they no longer generate highly uniform fields. This leads to signal fade-out and/or contrast change in larger field-of-view 3-tesla body images, although these effects vary from subject to subject.
In the new technology, individual RF coils may still not produce uniform fields, but this is neutralized by having multiple transmit channels, each of which can be controlled independently.
"With pTX, the field pattern can be changed to make the combined transmitter effect maximally homogeneous for each individual, just like changing the angle you hold a cup when you walk over a bumpy terrain so as not to spill its contents. This subject-specific adjustability is not achievable with a conventional fixed RF configuration," he commented.
A pTX system therefore allows the scanner to be customized to each subject and can produce increased fidelity in final images with more uniform signal and contrast. The system also provides radiologists with an opportunity for "trade-off."
"Because you can adjust performance, you can also reduce RF power deposition. This allows higher fidelity images to be obtained at current specific absorption ration (SAR) levels, or current quality images at lower energy dose or any chosen balance between the two," Hajnal said.
He pointed to an emerging approach in the research community to custom design individual RF pulses for each subject being scanned. "This can make full use of the new flexibility provided by pTX to create dynamically changing fields that may lead to new levels of performance," he noted.
Overall, there was also a clear but hidden statement in the discussion in Toulouse: 3-tesla machines are prone to severe image artifacts, and these artifacts can only be overcome by redesigning the existing systems. Widespread introduction of pTX MRI would require some redesign of scanners, and this would not be cheap, but there is a silver lining.
"Although this will undoubtedly entail an initial engineering effort on the part of manufacturers, the final systems need not be very different in cost from existing systems, as they are likely to have largely the same components but combined in a new way," Hajnal said.