In a comparison of hybrid imaging modalities, simultaneous whole-body PET/MRI is more accurate than retrospectively fused PET and MR images in abdominal organs and better than PET/CT in the urinary bladder, according to a German study published online on 8 May in Radiology.
Researchers from Eberhard Karls University in Tübingen found that simultaneous acquisition improved the alignment of abdominal organs between PET and MRI by 51%, on average, compared to a technique that used retrospectively fused images from the two modalities. Simultaneous PET/MRI also improved the alignment between morphological images and PET in the bladder by almost 50% compared to PET/CT images.
In addition, thoracic PET/MRI protocols with free breathing or an exhaling breath-hold improved alignment between MRI and PET by 60%, compared with PET/MRI where MR images were acquired while a patient inhaled.
The study was led by Dr. Cornelia Brendle, from the department of radiology and division of diagnostic and interventional radiology at the university (Radiology, May 8, 2013).
Imaging artifacts
Previous studies have shown that patient movement and organ motion caused by breathing, digestion, and other natural functions, along with time differences between image acquisitions with each modality, can cause misalignment of hybrid images, according to the authors.
Breathing motion often causes artifacts in organs in the upper abdomen and thorax, they noted. Past research suggests that different breathing protocols in whole-body PET/CT examinations favor the use of breath-hold CT in an exhaling or midbreath position, or CT with a free-breathing technique.
To evaluate the most effective approach with hybrid imaging, Brendle and colleagues compared the anatomic alignment between morphologic and PET images of the abdomen and pelvis using simultaneous PET/MRI, PET/CT, and retrospective PET/MRI fusion. They also hoped to assess alignment between images in simultaneous and sequential thoracic PET/MRI using different breathing, registration, and gating protocols.
The retrospective study included 35 patients with a clinical indication for whole-body FDG-PET/CT and a follow-up PET/MRI exam between April 2011 and January 2012.
The data included whole-abdomen and pelvis exams for 28 patients and whole-thorax imaging with different respiratory breathing protocols in seven patients. The mean patient age was 58 years, ranging from 21 to 75 years. The group consisted of 18 women (mean age, 56) and 17 men (mean age, 59).
The patients presented for their PET/CT scans with a variety of conditions, including lymphoma, cancer of the abdominal cavity, lung cancer, inflammation of unknown origin, esophageal cancer, and head and neck cancer.
The subjects received whole-body exams on integrated PET/CT scanners (Hi-Rez Biograph 16 and Biograph mCT, Siemens Healthcare). The scans included a whole-body CT protocol for attenuation correction and for diagnostic purposes, followed by PET acquisition from the skull base to midthigh. Subjects received a mean FDG dose of 347 MBq (± 20), with an uptake time of 61 minutes (± 6).
PET/MRI was performed on a simultaneous-acquisition hybrid system (Biograph mMR, Siemens), which combines a 3-tesla MRI scanner with a PET detector insert. The PET scan was acquired after an uptake time of 123 minutes (± 10), with a mean total scan time of 64 minutes (± 29).
Simultaneous MR images included 3D T1-weighted fast low-angle shot (FLASH) and coronal T2-weighted short-tau inversion recovery (STIR) sequences in the abdomen. In the thoracic region, coronal STIR and coronal T1-weighted 3D gradient-echo sequences were conducted.
Image alignment
For the abdominal regions, regardless of the modality, the researchers found the greatest image misalignments in the bladder (mean, 9.6 mm ± 6.6), followed by the liver (mean, 9.0 mm ± 5.6) and the spleen (mean, 8.7 mm ± 5.4).
The mean image misalignment was 5.8 mm (± 2.8) for all organs in simultaneous PET/MRI, compared with 7.2 mm (± 5.1) for PET/CT and 11.9 mm (± 6.3) for MR images retrospectively fused with PET data from PET/CT.
The analysis of single organs showed no significant differences between STIR PET/MRI and PET/CT in the upper abdominal organs, although STIR PET/MRI showed the least misalignment in the liver, spleen, and right kidney.
The alignment of all upper abdominal organs was significantly better with STIR PET/MRI than with sequential STIR PET/CT. In the bladder, the alignment was significantly more accurate with STIR PET/MRI than with PET/CT and sequential STIR PET/CT.
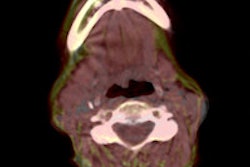
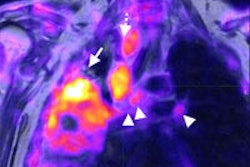
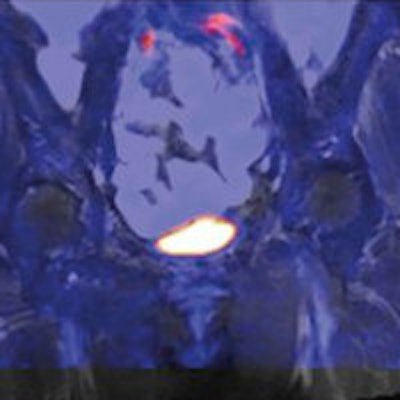
 Bladder of a 65-year-old female patient. Images illustrate improved alignment with simultaneous PET/MRI (A, coronal STIR; B, fused images) compared to sequential PET/CT (C, coronal CT; D, fused images) and retrospective fusion of PET and MRI (E, coronal STIR; F, fused images). Images courtesy of Radiology.
Bladder of a 65-year-old female patient. Images illustrate improved alignment with simultaneous PET/MRI (A, coronal STIR; B, fused images) compared to sequential PET/CT (C, coronal CT; D, fused images) and retrospective fusion of PET and MRI (E, coronal STIR; F, fused images). Images courtesy of Radiology.For all thoracic regions, the amount of misalignment was similar, according to Brendle and colleagues. Mean cumulative misalignment was 10.1 mm (± 7.7) in the right lung, 11.0 mm (± 8.4) in the left lung, and 12.0 mm (± 9.2) in the mediastinum.
As for the different breathing protocols, the overall alignment quality of the free-breathing and exhaling techniques did not differ significantly among the PET/MRI protocols.
However, the inspiratory PET/MRI protocol showed significantly worse alignment (24.5 mm ± 10.3) compared to the other breathing protocols for all thoracic regions and for each region separately (right lung, 23.4 mm; left lung, 23.7 mm; and mediastinum, 26.5 mm).
Study limitations
Brendle and colleagues cited several study limitations, including a small patient sample size.
"As a result, the lack of statistical significance of differences between certain imaging protocols or modalities may merely reflect the low statistical power of the study because of limited data, and not the lack of differences between the groups," the authors wrote.
Based on the results, the authors concluded that the alignment of hybrid datasets acquired in simultaneous PET/MRI was more accurate than with retrospective fusion for all abdominal organs. In addition, alignment with simultaneous PET/MRI was more accurate than with PET/CT in the urinary bladder.
"Appropriate thoracic PET/MRI protocols should include free-breathing or normal expiratory breath-hold MR," they added. "The possible benefit of MR-based motion correction of PET data combined with motion-corrected attenuation correction maps needs to be further evaluated."
Study disclosures
Eberhard Karls University has a collaboration agreement with Siemens regarding technical development of whole-body PET/MRI. However, the study stated that only authors with no industry affiliation had control over the data.