They require a little more contrast and dose, but catheterization procedures performed with flat-detector CT (FD-CT) offer high-resolution images that can improve the diagnosis of congenital heart disease in children by providing information that echocardiography and cardiac MRI cannot, according to a new study in European Radiology.
FD-CT, combined with image fusion to overlay 3D reconstructions on fluoroscopic images during catheter-based interventions, was useful -- and occasionally irreplaceable -- for deciphering the complex anatomy of congenital heart disease, wrote authors Dr. Martin Glöckler, Dr. Andreas Koch, and colleagues from University Hospital Erlangen in Erlangen, Germany.
"In particular, the possibility of acquiring 3D vascular volumes with high resolution and the option to visualize complex spatial relationships from any desired angle promises clinical utility to plan and guide interventional and surgical procedures," they wrote. (Eur. Radiol, 28 July 2011).



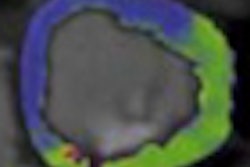
 A 6-year-old boy with transposition of the great arteries and arterial switch operation, Lecompte maneuver, patch enlargement of the central pulmonary arteries two years ago, former stent in the right pulmonary branch (star). Maximum intensity projection (MIP) picture B. Now balloon dilatation of peripheral pulmonary arteries stenosis, 3D-guided (D). All images courtesy of Dr. Martin Glöckler.
A 6-year-old boy with transposition of the great arteries and arterial switch operation, Lecompte maneuver, patch enlargement of the central pulmonary arteries two years ago, former stent in the right pulmonary branch (star). Maximum intensity projection (MIP) picture B. Now balloon dilatation of peripheral pulmonary arteries stenosis, 3D-guided (D). All images courtesy of Dr. Martin Glöckler."The fusion of 3D reconstructions with live fluoroscopic images during catheterization may help to find the ideal fluoroscopic angulation during catheter-based interventions, to achieve difficult vascular crossings by the wire or the catheter, to choose the most appropriate material for catheterization, and to define and control optimized positioning of implants such as stents or valve prostheses," Glöckler and colleagues explained.
To date, no standard protocols have been developed for the new technique. "Therefore we evaluated and report our experience in 62 consecutive cases [median age 3.5 years, 62% male, median weight 14.4 kg] in which FD-CT was applied in combination with standard fluoroscopy," they wrote.
The authors retrospectively analyzed patients in whom FD-CT was used during cardiac catheterization of congenital heart disease during 2010.
The exams were performed on a biplane angiography system equipped with two 20 x 20 cm2 flat-panel detectors with a 960 x 960 matrix (Axiom Artis, Siemens Healthcare). Images were acquired at a dose of 0.36 µGy per image (usually 30 but occasionally 60 images per second x five seconds) at 90 kV and automatically adapted tube current. The antiscatter grid was removed in patients less than 20 kg. Breathholding was used in the four patients with mechanical ventilation, the authors stated.
The researchers used a total of 350 mg/mL of contrast media (Imeron 350, Bracco Diagnostics) diluted with saline in a median concentration of 40%. Image acquisition was delayed after contrast medium injection by an amount of time that was adapted to the anatomical region, hemodynamics, and the site of injection.
A pediatric cardiologist reconstructed cross-sectional images at 0.4-mm thickness in a 250 x 250 matrix format on a Leonardo DynaCT workstation (Siemens Healthcare) immediately after acquisition. FD-CT was used for diagnostic purposes in 32 of 62 cases, for intervention in 30 of 62 cases.
If the surgery or the intervention required the additional information provided by FD-CT, the case was rated as "essential," they wrote. If the FD-CT added important information to what was already available the case was rated as "very useful." If useful information for preoperative planning or intervention is added but only minimally superior to the available information of angiographies, the case was rated as "useful."
The results showed that diagnostic utility was never rated as "misleading," however, FD-CT was classified as "not useful" in six cases (9.7%), "useful" in 18 (29%), "very useful" in 37 cases (59.7%), and "essential" in one case (1.6%). Compared with traditional angiography, the median added dose-area product was 111.0 µGym2, and the mean additional quantity of contrast was 1.6 mL/kg.



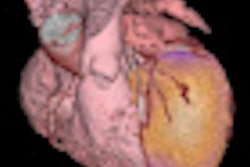
 Forty-year-old woman with transposition of the great arteries, Senning operation. Now total superior vena cava obstruction (arrow), venous drainage over large azygos vein (star). Implantation of a stent in the upper venous baffle after needle-perforation, 3D-guided (C+D).
Forty-year-old woman with transposition of the great arteries, Senning operation. Now total superior vena cava obstruction (arrow), venous drainage over large azygos vein (star). Implantation of a stent in the upper venous baffle after needle-perforation, 3D-guided (C+D)."One unique feature of FD-CT is the possibility of merging 3D reconstructions with the real-time fluoroscopic image," a potentially useful way to identify ideal C-arm angulations for achieving wire passage for atypical vascular crossings, and to optimally depict the implant position of coils, plugs, stents, and valves," Glöckler and colleagues wrote. "In fact, image fusion of 3D reconstructed FD-CT images with the live fluoroscopic image was frequently rated as 'very useful' (57.4%)."
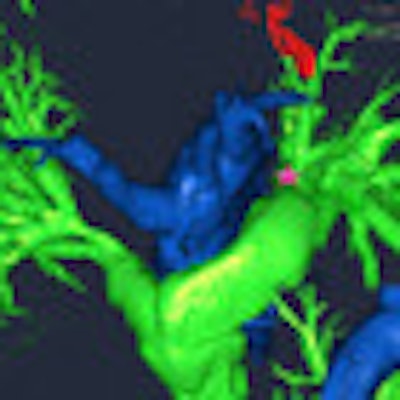
A typical example is the visualization of the coronary arteries during transcatheter pulmonary valve implantation.
"Although cardiac ultrasound is the standard for preoperative imaging in most cases of congenital heart disease, there may be remaining questions in several situations that cannot be answered by echocardiography," the authors wrote. "They may be due to bad acoustic windows, superposition of air, or difficult spatial relationships of cardiac and vascular structures."
For its part, cardiac MRI can assess the dimension, structure, and function of the ventricles, including myocardial abnormalities such as late enhancement, as well as assess valve function and anatomy of the great vessels and with limitations even the coronary arteries.
As a new technology, FD-CT also offers 3D imaging during cardiac catheterization, a clear extension of available imaging techniques, and the technique could also be useful for the assessment of valve function and great vessel anatomy, the group reported.
"FD-CT imaging in the context of invasive catheterization has so far mainly been used in neuroradiology, tumor embolization, apical aortic valve replacement in adults, as well as in electrophysiology interventions," the authors wrote.
In congenital heart disease, the need for 3D information is significant for use in surgical and interventional planning, they wrote. The evolution of MDCT makes that modality a contender as well, providing high-resolution images even in neonates.
Still, FD-CT has an advantage "in its immediate availability during the invasive investigation in the catheterization laboratory," the authors wrote. "3D reconstructions of cardiac and vascular anatomy can be performed almost in real-time and are available for immediate use in the same setting."
The authors said they rated the success rate and diagnostic utility of FD-CT higher than the authors of the only other study of congenital heart disease, Glatz et al -- possibly due to differences in the clinical characteristics of the patients and/or the learning curve for the new technology, the authors stated.
The technology is new, and needs experience with different protocols -- especially low-dose protocols -- to optimize results, and therefore needs additional studies, Glöckler and colleagues wrote. In particular, randomized studies with conventional invasive angiography are needed to define the role of this new modality.
The principal limitation of the study was that patients were not randomly assigned to different image modalities; therefore no direct comparison is possible. In addition, the image-quality assessments were not objective.
The use of FD-CT during catheterization of congenital heart disease "provides diagnostically useful information and is not associated with unreasonable added radiation or contrast medium exposure," the group concluded. "According to our experience in 62 patients, the main advantages of this new imaging technique include the acquisition of high-resolution 3D vascular models for surgical planning and the use of these models in interventions during the same investigation."