Patient selection, preparation, and assessment are the vital considerations to ensure image optimization in cardiac CT, according Dr. James Stirrup, clinical research fellow in cardiac imaging at London's Royal Brompton Hospital.
It is important to select patients who are appropriate, according to the criteria for CT, and to exclude patients when CT is not considered the best modality for them, he told delegates at the recent British Institute of Radiology (BIR) President's Conference in London.
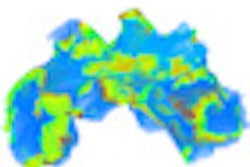
 The effect of poor-quality ECG amplitude is seen on the left image, with clear artifact compromising image quality. The R and T waves are of equal amplitude, resulting in images derived from imaging data combined from two separate phases of the cardiac cycle. Editing the ECG gating (right) so that only one phase from each cardiac cycle is used to reconstruct the images largely eliminates the artifact. All images courtesy of Dr. James Stirrup.
The effect of poor-quality ECG amplitude is seen on the left image, with clear artifact compromising image quality. The R and T waves are of equal amplitude, resulting in images derived from imaging data combined from two separate phases of the cardiac cycle. Editing the ECG gating (right) so that only one phase from each cardiac cycle is used to reconstruct the images largely eliminates the artifact. All images courtesy of Dr. James Stirrup.Patient weight is related directly to the scan quality, and the heavier the patient, the greater is the likelihood that the scan will be of poorer quality, Stirrup noted. Diagnostic accuracy is reduced in obese patients because the scan beam is significantly more attenuated as a result of increased tissue between the tube and the detectors; this is especially important when looking at small vessels. Image quality in patients who have a lot of calcium also may be reduced, particularly if narrowing of the vessels is under investigation. He advocates using beta-blockade to improve image quality for all patients regardless of CT scanner technology. Scanning those who have poorly controlled atrial fibrillation often results in a poor-quality image and such patients are often better served by an alternative imaging technique.
To improve image quality in overweight patients, tube voltage can be increased to boost beam energy, but this is limited by the amount of energy that can be put through an x-ray tube. For contrast issues, Strirrup suggests higher flow rates or stronger contrast agents may be more suitable for overweight patients.
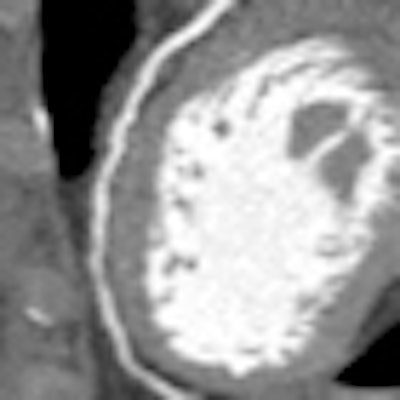
 Kernel selection has an important effect on final image quality, especially in the presence of significant calcification or coronary stenting. The image on the left shows a curved multiplanar reformat of a stented coronary artery reconstructed using a medium-smooth kernel. This results in significant blooming artifact and precludes adequate diagnostic assessment. Reconstructing the same dataset using a medium-sharp kernel reduces stent blooming and allows assessment of the stent lumen.
Kernel selection has an important effect on final image quality, especially in the presence of significant calcification or coronary stenting. The image on the left shows a curved multiplanar reformat of a stented coronary artery reconstructed using a medium-smooth kernel. This results in significant blooming artifact and precludes adequate diagnostic assessment. Reconstructing the same dataset using a medium-sharp kernel reduces stent blooming and allows assessment of the stent lumen.Well-informed patients are likely to be compliant and do what is required of them, which is important to reduce respiratory motion artifacts. Teaching breath-holding exercises whilst patients are in the gantry is an important part of patient preparation, not only to reduce respiratory motion artifacts but also to enable the physician to see the heart rate during breath-holding sequences. If the heart rate is reduced during this time, it will be easier to perform the scan, and it may not be necessary to perform rate control, noted Stirrup, who cautions against using the Valsalva maneuver as this causes unpredictable changes in heart rate.
|
Checklist for ensuring image quality
Source: Dr. James Stirrup, BIR President's 2011 Conference |
Heart rate control and fast gantry rotation time are important to perform single heartbeat acquisition scans, and the extent to which patients require beta-blockade/rate control depends on the scanner. Likewise, the choices for different rate control options can vary; e.g., glyceryl trinitrate (GTN) is popular in the U.S. for imaging distal coronary arteries because it is a potent vasodilator and improves opacity. Indications for use would be those patients who may have a predisposition to small vessel disease, such as smokers and diabetics. Stirrup recommends using a pro forma to document all procedural aspects, including heart rate control and any breath-holding sequences (and their effects) that need to be used during imaging.
"It is also important to get a good amplitude R wave when looking at optimizing images with correlated ECG, despite the fact that ECG leads need to be kept out of the area of interest," said Stirrup, who recommends placing pads on each shoulder and on the abdomen.
To obtain the single heartbeat acquisition scan needed, he suggests using a large cannula needle that will allow fast flow rates for injection of contrast medium. The right antecubital fossa is the preferred place for placing the cannula because the contrast reaches the heart without crossing the aortic arch, reducing the chance of streak artifacts.
Note: Some of the information presented by Dr. Stirrup at the BIR President's Conference, including the images, have come from the forthcoming Oxford Handbook of Cardiovascular Computed Tomography (Nicol E, Stirrup J, Padley S, Kelion A, eds., Oxford University Publishing, 2011).