Dedicated breast CT has long been proffered as a potential rival to mammography for breast screening, but early prototype systems have been limited by higher radiation dose and lower resolution. In a new paper in European Radiology, however, German researchers report progress in addressing both concerns.
Researchers are always looking for newer and better ways of detecting breast cancer early and reliably. Full-field digital mammography, breast MRI, and digital breast tomosynthesis are currently used, but they're not without their drawbacks, such as digital mammography's variable sensitivity for identifying lesions, tomosynthesis' limited depth information, and MRI's poor calcification detection.
 Willi Kalender, PhD, and his team at Erlangen are conducting some important research on breast CT.
Willi Kalender, PhD, and his team at Erlangen are conducting some important research on breast CT.
Dedicated breast CT may eventually provide an alternative through comprehensive diagnostic assessment of microcalcifications and soft-tissue structures at dose levels equal to or below two-view screening mammography, according to a study led by CT pioneer Willi Kalender, PhD, professor and chairman of the Institute of Medical Physics at the Friedrich-Alexander-University of Erlangen-Nuremberg in Germany (Eur Radiol, 9 June 2011).
According to the authors, the "perfect" breast imaging modality should have the following:
- Full 3D capability
- Good soft-tissue differentiation
- Accurate tissue density assessment
- Dynamic contrast-enhanced imaging
- High isotropic spatial resolution of 100 microns
- Low patient dose with an average glandular dose below 5 mGy
- The ability to keep a patient comfortable without breast compression
- An integrated biopsy option
- Low cost
CT is a candidate because of its 3D capability, adequate soft-tissue differentiation, local tissue density values, and contrast-enhanced imaging, he wrote. The problems with CT are high resolution and good lesion detection in a single low-dose acquisition.
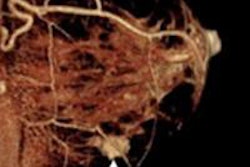
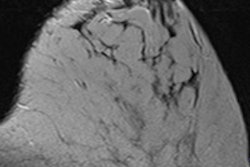
What Kalender and his team found is by micro-CT imaging of specimens, CT with high isotropic spatial resolution can provide the resolution for excellent assessment of microcalcifications with a signal above 5,000 HU at 60 kV. They have developed a dedicated breast CT system with cadmium telluride (CdTe) crystals and photon-counting electronics with 100-micron detector element size for close to 100% dose efficiency. They assessed the potential for imaging microcalcifications of 100 microns to 200 microns in diameter, and soft-tissue lesions between 1 mm to 5 mm in diameter, by simulations at dose levels between 1 mGy and 6 mGy.
Using the new technique, the researchers clearly detected microcalcifications of 150 microns and soft-tissue lesions of 2 mm in diameter at an average glandular dose of 3 mGy. Separate displays are required for high-resolution microcalcification and for low-resolution soft-tissue analysis, they wrote. In addition, total CT data acquisition time was below 10 seconds.
Due to the system's high signal (60 kV), the existence of microcalcification clusters is clearly recognizable even when they are not resolved as single entities, Kalender wrote. He suggests starting with a very low-dose overview CT data acquisition and following up with high-resolution CT of a limited volume of interest.
"We have shown that this general approach can provide high resolution with reduced total dose," he wrote. "Even the standard single-CT data acquisition approach appears to provide detectability of microcalcifications superior to mammography, which may claim about 150 μm at best."
The results of the study also indicate CT will not need dose levels higher than those associated with mammography screening, the researchers stated.
"Our favorable results have to be assigned to a strict optimization strategy with respect to dose efficiency: It relates to the choice and design of the components, primarily to the directly converting CdTe detector, to the spiral scan geometry, and to the versatile image reconstruction, and data handling approach," they wrote.
According to the researchers, dedicated breast CT seems to be a good candidate for the "perfect" breast modality for the following reasons:
- Excellent spatial resolution of down to 100 microns was shown to be achievable -- with further reductions possible in situations in which high resolution is not required.
- Dose levels below the upper level of 5 mGy are realistic.
- Soft-tissue lesion detection well below a diameter of 5 mm appears possible with and without contrast media.
- Areas of microcalcification are easily detected as clusters even in the soft-tissue displays.
- Single microcalcified foci are visible down to a diameter of 150 microns.
Experimental and clinical proof of the novel technique's performance is planned for late 2011 and 2012, the researchers noted.