High-pitch chest imaging with dual-source CT (DSCT) is robust enough to image the coronary arteries in many patients -- despite fast heart rates and nongated CT acquisitions, according to a study conducted by a French group that included Dr. Martine Rémy-Jardin.
Rémy-Jardin led a group from Hôpital Calmette in Lille, France, that used a high-pitch scan mode on two models of dual-source CT scanners in nearly 300 patients. Results were presented at the 2011 ECR.
With the advent of 64-detector-row CT, it has become possible to sometimes include the evaluation of coronary arteries and cardiac function from chest exams, Rémy-Jardin said in her ECR presentation.
In fact, there are several clinical situations in which the additional information from a chest scan can be very helpful for evaluating the cause of the patient's complaints, she said. Originally, evaluation of coronary arteries in chest CT was proposed for patients with dyspnea using retrospective gating, Rémy-Jardin said.
"[In DSCT] we have high-pitch scanning mode, which offers the option to integrate vessels into the chest CT examination," she said. "However, to our knowledge this technique was mainly applied to patients who had an exam acquired with prospective [electrocardiogram (ECG)] gating."
In their study, Dr. M. de Malherbe, Rémy-Jardin, and colleagues aimed to evaluate the assessability of coronary arteries on DSCT studies in high-pitch mode in patients who had neither ECG synchronization or beta-blockade in the protocol.
The study evaluated 242 "mostly oncology" patients using a nongated CT angiographic examination of the chest. Dual-source single-energy CT was obtained with a pitch of 3 and a temporal resolution of 83 msec (Somatom Definition, Siemens Healthcare; group 1, n = 116) or 75 msec (Somatom Definition Flash, Siemens; group 2, n = 126).

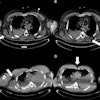
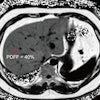
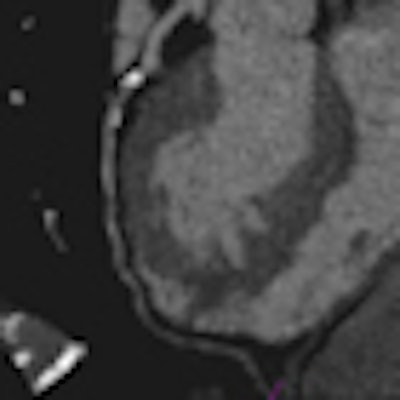
 Images of a 65-year-old male patient acquired in dual-source CT high-pitch mode show good enhancement of the coronary arteries down to their distal portions. Top image shows calcified stenosis at the origin of the proximal portion of the left anterior descending (LAD) artery.Bottom image depicts the left circumflex (LCX) artery, and an absence of atherosclerotic lesions. The acquisition consisted of a whole-chest CT angiography exam obtained without beta blockers or electrocardiac gating. All images courtesy of Dr. Martine Rémy-Jardin.
Images of a 65-year-old male patient acquired in dual-source CT high-pitch mode show good enhancement of the coronary arteries down to their distal portions. Top image shows calcified stenosis at the origin of the proximal portion of the left anterior descending (LAD) artery.Bottom image depicts the left circumflex (LCX) artery, and an absence of atherosclerotic lesions. The acquisition consisted of a whole-chest CT angiography exam obtained without beta blockers or electrocardiac gating. All images courtesy of Dr. Martine Rémy-Jardin.Collimation was set thin at 0.6 mm, and protocols for both machines used individually adapted selection of kVp for tubes A and B, at 100 kVp (body weight < 80 kg) or 120 kVp (body weight 80-120 kg). Automatic adjustment was achieved using CareDose (Siemens) with a reference setting of 90 mAs.
Reconstruction parameters included a second series of images for coronary artery assessment using a small field-of-view and soft-tissue kernel. Coronary artery images included multiplanar reconstructions (MPRs) and maximum-intensity projection images (MIPs) using cardiac CT visualization software.
In all, 116 consecutive patients were imaged on the Definition scanner and 126 on the commercial-model Definition Flash.
"Most of our interest as cardiovascular radiologists is at the level of the proximal and midsegments," Rémy-Jardin said. The mean level of attenuation within the proximal segments was 333.3 ± 63.3 HU. A minimum HU level of 200 was one of the requirements for considering a vessel as being assessable.
Coronary artery imaging per-vessel analysis
|
Percentage of patients with assessable coronary segments
|
"Results were excellent for the study population of 242 patients," she said. The two groups had about equal heart rates (mean, 82.6 bpm) and no significant differences in patient categories at evaluation, she said.
"In the vessel-by-vessel analysis, 88% of proximal segments were assessable, 75% of proximal and midsegments, and only 48% for the entire coronary artery tree, without significant differences between group 1 and group 2," she said.
In the per-patient analysis, 67% were assessable in the proximal segments but just 23% in the proximal and midsegments.
"Diagnostic image quality was obtained in a high proportion of patients in the proximal segments -- and some segments were particularly well-evaluated," Rémy-Jardin said. "We have to point out that scanning conditions of the study were really very different from those of gated cardiac CT studies, considering the high heart rate, the lack of ECG-gated acquisitions, and the parameters which were very standard for chest examinations."
This kind of imaging protocol is certainly justifiable for patients in whom no interest is foreseen in evaluating the coronary arteries, she said. Still, "for perspective we should probably look at the possibility of reconsidering the acquisition in selected [chronic obstructive pulmonary disease (COPD)] patients to improve the results with prospective ECG gating," Rémy-Jardin said.
Unfortunately, beta-blockers are not recommended in COPD patients, for example, so the fast heart rates aren't an issue that will be easily resolved.