A national survey of scan protocol behavior and radiation dose at hospitals in Belgium has found that even though most facilities are generally keeping pediatric CT radiation dose low, there is still some variation between sites in terms of median dose levels.
Researchers surveyed 21 CT departments in seven university hospitals and eleven community hospitals. Ninety percent used either 64-slice (47%) or 16-slice (43%) CT scanners and 10% used four-slice systems. All were equipped with automated tube current modulation (ATM) systems. The exams for which data were collected included head, sinus, inner ear, chest, and abdominal CT for four pediatric age groups: birth to 12 months, 5 years, 10 years, and 15 years.
The findings were presented at the 2009 RSNA meeting by Nico Buls, Ph.D., a medical physicist at Universitair Ziekenhuis Brussel. The survey was funded by the Belgian Federal Agency for Nuclear Control.
A certified medical physicist visited each center to record scan protocols and measure CT dose index volume (CTDIvol) and dose-length product (DLP) in a 16-cm dosimetric phantom during 2007 and 2008. A total of 161 different protocols were identified. All of the centers adapted technical scan parameters for pediatric exams, with 47% adapted to age, 24% adapted to weight, and 29% using a general protocol.
Observed median doses for all CT exams and age groups studied were below published international diagnostic reference levels. However, doses for infants varied up to a factor of 15 among centers for the same exam, and 10% of the individual protocols exceeded diagnostic reference levels.
The researchers found that 10% of sites used a reduced tube voltage of less than 120 kV for head CT exams, 38% for chest CT exams, and 36% for abdominal CT exams. ATM was only applied in 47% of the protocols, with the remainder using fixed tube currents to achieve lower doses.
Buls and colleagues reported shortcomings in the use of ATM for dose reduction.
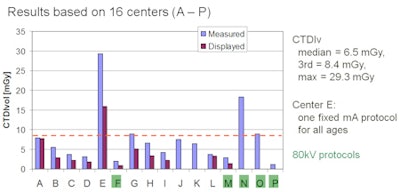
"The results of this study showed that the highest doses were observed with centers that use a scan protocol with high default ATM dose setting for children of all ages, regardless of their body size," according to the group. "This methodology specifically resulted in high doses for the two youngest age groups."
The regulation of the ATM depends on the type of CT scanner used, they continued. During visits to perform the dose audits, the researchers discovered that some CT radiographers were not very familiar or experienced in presetting the ATM system, and it often is a source of confusion.
As part of the dose audit, each ATM system was tested by scanning two phantom sizes. Most systems automatically reduced radiation dose, with a median reduction of 34%, but for some systems there was no dose reduction whatsoever, according to Buls.
"ATM systems cannot be treated as a 'plug and play' utility for dose control," Buls cautioned. "While ATM systems can be a helpful radiation protection tool, it does not automatically scan the patient with an appropriate dose, especially for the youngest age groups."
 |
| Dosimetry results: Chest, 0-1 year. Images courtesy of Nico Buls, Ph.D., Universitair Ziekenhuis Brussel. |
 |
| Dosimetry results: Head, 0-1 year. |
The research team believes that the data show an encouraging trend toward adequate radiation protection management of pediatric CT dose. The team plans to make study results available to individual centers and to recommend changes to improve dose optimization.
"I think that the attention that has been given in the past five to 10 years to radiation protection has definitely resulted in more adequate use of CT scanning in clinical practice," Buls told AuntMinnie.com. "This is due to a combination of technical radiation protection tools and increased awareness of the users."
"I think this is very crucial," he continued. "Radiation protection methods can be developed, and promising results can be reported by the media and in journals. However, this does not guarantee that the result is a dose reduction in clinical practice."
By Cynthia E. Keen
AuntMinnie.com staff writer
April 23, 2010
Related Reading
Reduced dose can still yield acceptable pediatric CT images, April 22, 2010
Automated exposure control delivers uneven CT dose reduction, April 15, 2010
Low-dose CT may be suitable for pediatric fracture diagnosis, March 7, 2010
CT doses, widely variable in Europe, are reduced by staff efforts, March 6, 2010
320-row CT minimizes dose in pediatric abdominal studies, March 3, 2010
Copyright © 2010 AuntMinnie.com


















