Researchers from France have found that whole-body dynamic contrast-enhanced MRI can help assess treatment response in patients receiving stem cell therapy for multiple myeloma by providing quantitative analysis of bone marrow and focal lesion enhancement.
The additional patient information, the authors wrote, "may help detect residual disease following high-dose therapy and autologous stem cell transplantation and help identify patients who might benefit from therapy modification."
The research from the University of Paris in Créteil, France, and Hôpital Européen Georges Pompidou in Paris was published in the February issue of Radiology, with Dr. Chieh Lin from the University of Paris as the lead author (2010, Vol. 254:2, pp. 521-531).
According to previous research, bone marrow biopsy detects higher microvessel density in patients with newly diagnosed multiple myeloma compared to normal subjects. With appropriate therapy, microvessel density can decrease, reducing the chance of disease progression.
The authors cited a 2009 Dutch study that concluded whole-body MRI, even without contrast, is more accurate than skeletal x-ray, whole-body MDCT, and PET for staging multiple myeloma. In that study, whole-body MRI helped to identify additional lesions in 30% of patients with multiple myeloma and altered the treatment plan in half of those patients.
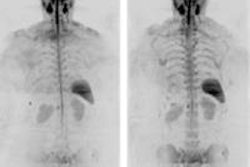
With that background, the researchers used whole-body dynamic contrast-enhanced MRI to compare post-treatment bone marrow changes with the clinical response in patients with multiple myeloma to determine if this technique can be used to assess treatment response.
The researchers prospectively enrolled 30 patients in the study between December 2006 and November 2008. All 30 patients received 1.5-tesla whole-body dynamic contrast-enhanced MR imaging (Magnetom Avanto, Siemens Healthcare, Erlangen, Germany) before and after treatment for their myeloma.
The group included 21 men and nine women, with a mean age of 58 years, ranging from 34 to 79 years. A total of 80 MRI exams were performed in the 30 patients. Two radiologists analyzed the images in consensus, unaware of the patient treatment response and the patients' clinical data except for his or her age.
A baseline MRI scan was taken in all 30 patients prior to chemotherapy or autologous stem cell transplantation (ASCT), with follow-up MRI exams one month after completion of chemotherapy in all 30 patients, after several chemotherapy treatments in three patients older than 65 who did not qualify for ASCT, and a follow-up two to four months after ASCT in 20 patients.
Patients' clinical results then were monitored every three months for the first year of the study, and then every six months in the following years.
Good, bad responders
The study also classified the 30 patients as either good responders or poor responders relative to their treatment. A "good responder" was defined as a patient with complete response or very good partial response after treatment, as they likely would have significantly longer overall survival than patients with only partial response to treatment. Patients with partial response, stable disease, or progressive disease were considered "poor responders."
The evaluations determined that 11 of the 30 patients had a good clinical response to chemotherapy, with seven complete responses and four very good partial responses. The remaining 19 patients were considered poor responders, with seven partial responses, seven patients with stable disease, and five patients whose disease had progressed.
The researchers noted that prior to treatment, the MRI pattern of bone marrow infiltration was abnormal in all patients, with 11 patients (37%) having focal lesions, five patients (16%) with diffuse infiltration, and 14 patients (47%) with both diffuse infiltration and focal lesions.
No change was found in MRI patterns of bone marrow infiltration after chemotherapy treatment in any of the 30 patients. Bone marrow T1 signal also remained unchanged in 11 good responders, which included six patients with persistent diffuse infiltration, all of whom had focal lesions at baseline MR examinations.
Lesion detection
The number of focal lesions decreased in 10 patients and remained unchanged in one case. Bone marrow T1 signal remained unchanged in 18 of 19 poor responders. The number of focal lesions decreased in five of 14 patients with focal lesions and was unchanged in nine.
After stem cell transplantation, bone marrow T1 signal was unchanged in nine of 16 good responders. Bone marrow T1 signal normalized after ASCT in seven (70%) of 10 patients who had diffuse infiltration before treatment. The number of focal lesions decreased in 13 of the 14 patients with focal lesions and remained unchanged in one.
Among the four poor responders, bone marrow T1 signal remained unchanged in three patients and normalized in one other case. The number of focal lesions decreased in all three patients with focal lesions.
The researchers also assessed the maximal percentages of bone marrow (BMEmax) and focal lesion (FLEmax) enhancement for each MRI scan. The mean baseline BMEmax in all 30 patients was 157.0%, with a range of 76.6% to 289.7%.
After the start of chemotherapy, the mean BMEmax differed between good and poor responders by 94.3% to 138.4%, respectively.
Clinical response
With the exclusion of results from six examinations with focal lesions in which a poor clinical response was classified, but BMEmax had normalized, results for patients with a post-treatment BMEmax of more than 96.8% had 100% sensitivity for the identification of poor responders.
After ASCT, the mean BMEmax in the 20 studied patients decreased to 90.2%, with a range of 85.5% in the 16 good responders to 107.5% in the four poor responders.
With baseline examinations having shown 105 focal lesions, the mean FLEmax of those lesions was 242.6%. After induction chemotherapy, FLEmax was 161.9%, with a range of 145.5% in 11 good responders to 175.4% in 14 poor responders.
After treatment via ASCT, FLEmax was 64.3% in 17 patients with focal lesions, 69.8% in 14 good responders, and 28.8% among the three poor responders.
Study limitations
The authors cited several limitations of the study. They noted that the 30 patients in the study groups did "not have an identical treatment protocol. Our study was not aimed to assess the efficacy of a specific treatment strategy but rather to show that monitoring treatment response in patients with multiple myeloma with this technique was feasible."
Another limitation was the relatively small sample of 30 patients and that consensus reading for image analysis did not allow evaluation of interobserver variability.
Despite the limitations, the researchers concluded that whole-body dynamic contrast-enhanced MRI "can be used to assess treatment response in patients with multiple myeloma. It may also be useful for early detection of disease progression after ASCT."
By Wayne Forrest
AuntMinnie.com staff writer
February 11, 2010
Related Reading
New progress in multiple myeloma treatment; MDCT has edge in detection, June 18, 2007
High-dose therapy does not improve multiple myeloma outcome, March 9, 2006
No survival benefit of high-dose therapy in multiple myeloma, January 5, 2006
Copyright © 2010 AuntMinnie.com