Computer-aided detection (CAD) can improve the performance of experienced radiologists in detecting intermediate-sized (6- to 9-mm) polyps, but it doesn't help find larger lesions, said researchers from Italy in results presented at the RSNA meeting earlier this month.
The 10-center trial, dubbed CAD-IMPACT, examined more than 600 higher-risk screening subjects who underwent virtual colonoscopy (also known as CT colonography or CTC) as part of a nationwide VC screening study published this year and first reported by AuntMinnie.com in 2007.
Although computer-aided detection schemes have been used in different reading paradigms, including both experienced and inexperienced readers, there are "no data available on CAD performance in a prospective setting and in a real clinical environment," said lead author Dr. Daniele Regge from the Institute for Cancer Research and Treatment in Turin, Italy.
The evidence shows that CAD can boost results in virtual colonoscopy reading. Radiologists can use the help, especially for difficult-to-detect lesions. Overall, approximately half of all misses are due to observer error -- and three-quarters of misses are polyps in the intermediate range, Regge said. The 6- to 9-mm lesions are worth finding, because about one-fourth of them are advanced, he added.
"The study aimed to assess if CAD-assisted reading increases detection of medium-sized polyps in comparison to nonassisted reading," Regge said in his RSNA talk. "The secondary aim was to determine the per-polyp sensitivity" of CAD as a second reader.
Regge, along with Patrizia Della Monica, Ph.D., Dr. Cristiana Laudi, Dr. Alberto Bert, and other colleagues, examined a total of 651 individuals in cooperation with researchers from CAD developer im3D of Turin, Italy.
 |
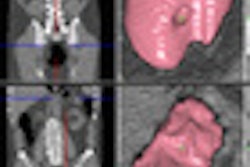
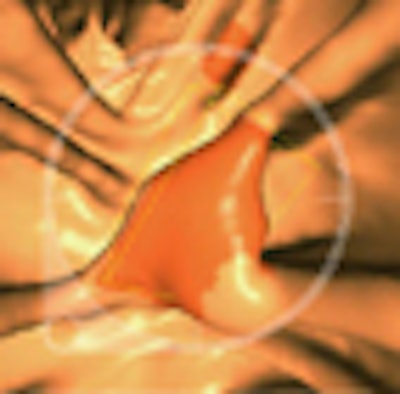
| In a 59-year-old man, a 6-mm sessile polyp on a haustral fold visible only on the prone scan was missed by the radiologist but found by CAD. Histology: hyperplastic. All images courtesy of Dr. Daniele Regge. |
All CTC studies were performed using cathartic bowel preparation and a low-dose protocol. Exams were read by an experienced radiologist unassisted, and then with the aid of a commercial CAD system (CAD-Colon, im3D).
"Each center had a CAD workstation customized for the study," Regge said. Enrollment criteria for the mostly higher-risk patients included:
- Age 50 years or older
- Age 40 years or older with a family history of colorectal cancer
- Age 18 years or older with a personal history of polyps and cancer
- Any age with a positive result on fecal occult blood testing
"We expected about a prevalence of 10% of patients with [one or two 6-to 9-mm polyps], and we hypothesized increased sensitivity in this population of about 15% with CAD," Regge said.
All patients underwent cathartic bowel cleansing using a regimen of polyethylene glycol only (six centers, n = 244), or a sodium phosphate preparation with the iodinated oral agent gastrografin for tagging (four centers, n = 374). Only expert CTC readers interpreted the results, Regge said.
The reference standard was unblinded conventional colonoscopy and histology. The researchers calculated per-polyp sensitivity for polyps in different size categories (≥ 6 mm, ≥ 10 mm, and 6-9 mm), he said. The sensitivity of unassisted reading was compared to that of CAD-aided interpretation. Differences between the tests were compared using McNemar's test.
Of the 651 individuals enrolled between July 2007 and March 2009, a few were excluded or dropped out, leaving a cohort of 618 (337 men) with a mean age of 59 years. Of these, 464 were negative at CTC and colonoscopy, 80 had colorectal lesions 10 mm or larger, and 52 had only 6- to 9-mm lesions -- the group that formed the heart of the CAD analysis. Twenty-two cases of colorectal cancer were detected by the radiologists, CAD, and conventional colonoscopy, Regge said.
Patients in the study cohort were referred for screening for the following reasons:
- Family history (n = 282)
- Symptoms (n = 103)
- Positive fecal occult blood test (n = 91)
- Average risk (n = 78)
- Personal history (n = 64)
"In the per-patient analysis, we got improvement in sensitivity from 65% to 77% for 6- to 9-mm lesions," Regge said. "That means CAD identified six additional patients with 6- to 9-mm polyps. But patients with larger lesions had no benefit from CAD. And if you divide the patients into fecal tagging and no fecal tagging, you see that CAD is useful [only] for the fecal tagging population."
For lesions 10 mm or larger, per-patient sensitivity was 93% both before and after the CAD algorithm was applied. CAD significantly increased sensitivity in the fecal tagging population, from 57% to 71% (p = 0.0253), but improvement from 82% to 88% in the nontagged individuals was not significant (p = 0.3173).
 |
| Above, per-patient performance results segregated by bowel prep regimen show significantly improved sensitivity in individuals with 6- to 9-mm lesions who underwent fecal tagging. Below, combined results for detecting adenomas and hyperplastic polyps in all patients again demonstrate significant improvement only in individuals with 6- to 9-mm polyps. |
 |
Among 99 polyps measuring 6 to 9 mm in diameter, 64 (65%) were detected by the reader alone, with an additional nine detected only with the addition of CAD, Regge reported. A total of 12 true-positive CAD marks were rejected by readers, and six 6- to 9-mm lesions were seen by neither the readers nor the CAD and were reconciled only retrospectively.
CAD also reduced reading time, from an average four minutes, 50 seconds, down to one minute, 29 seconds, in tagged data; and from 11 minutes, 47 seconds, to three minutes, 59 seconds, in untagged data.
"CAD improves the detection of polyps in the 6- to 9-mm range; however, 12% of intermediate-sized polyps found by CAD are rejected by the radiologist," Regge concluded. "CAD is not helpful for lesions larger than 10 mm, and CAD does not affect specificity."
By Eric Barnes
AuntMinnie.com staff writer
December 28, 2009
Related Reading
CAD catches most flat polyps on virtual colonoscopy, December 16, 2009
Virtual colonoscopy effective in higher-risk subjects, June 16, 2009
Virtual colonoscopy CAD improves flat-lesion detection, June 5, 2009
ACRIN trial shows VC accuracy comparable to optical colonoscopy, September 18, 2008
Italian multicenter VC trial screens higher-risk cohort, October 17, 2007
Copyright © 2009 AuntMinnie.com