Researchers from the U.K. and Australia are reporting early success with a PET/MRI-based motion correction model that, so far, has significantly improved the detection of cancer, according to a study published in the September issue of the Journal of Nuclear Medicine.
"We have demonstrated significant improvements in quantification and detection of PET-avid lesions using multiple tracers and in multiple organ locations, with specific case examples showing where motion correction has the potential to affect diagnosis or patient care," wrote the researchers led by Dr. Richard Manber from the Centre for Medical Imaging at University College London.
One drawback of PET is the length of time a patient must remain still while technologists acquire a variety of images, with acquisition times generally ranging from three to 15 minutes per bed position, according to the group. The modality already has limited spatial resolution, and patient motion can further blur results and cause errors in quantification.
Manber and colleagues therefore sought to develop a method of respiratory motion correction using a predictive motion model that features one minute of simultaneous acquisition by PET and MRI (Biograph mMR, Siemens Healthineers). The goal was to capture cyclical breathing variations and use that data to adjust for patient motion (JNM, September 2018, Vol. 59:9, pp. 1467-1473).
The researchers retrospectively analyzed 42 patients (mean age, 61.9 years; range: 36-85 years) who had undergone PET/MRI scans between February 2014 and November 2015. Twenty-four patients received FDG, while 18 were given gallium-68 DOTATATE. PET/MRI protocols included an additional breath-hold Dixon MRI sequence for PET attenuation correction and a one-minute free-breathing dynamic MRI sequence.
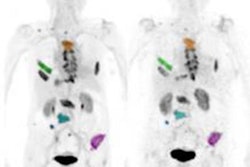
In their review of uncorrected and motion-corrected images, two radiologists found 162 PET-positive lesions in the liver, pancreas, kidney, bowel, rib, and shoulder among 32 patients. There were no detectable lesions among the other 10 subjects.
The radiologists achieved greater average sensitivity with the motion-corrected images (84%) than the uncorrected images (74%). In addition, the number of false-positive lesions decreased from 30 with the uncorrected images to 21 with motion correction. Peak standardized uptake values (SUVpeak) and maximum SUV (SUVmax) also increased with motion correction, as did the radiologists' confidence on a four-point scale.
| Effects of PET/MRI motion correction | |||
| Uncorrected | Motion-corrected | p-value | |
| SUVpeak | 17.6 ± 18.0 | 19.5 ± 20.1 | < 0.0001 |
| SUVmax | 22.7 ± 22.6 | 26.6 ± 29.9 | < 0.002 |
| Average sensitivity | 74% | 84% | NA |
| No. of false-positive lesions | 30 | 21 | NA |
| Mean confidence score | 2.67 | 3.01 | < 0.0001 |
Study limitations included intra- and interobserver variability, as well as the lack of a definitive method for identifying false positives, the authors noted.
"These lesions were marked as [false positives] because evidence of a true lesion was lacking in the patient information or in the results of other imaging modalities, but in reality, some of these [false positives] may have been real lesions," they wrote.
"We consider this study a pilot analysis of our method," Manber and colleagues concluded. "With a streamlined pipeline and enhanced data processing efficiency, the method can be adopted into routine practice, which in turn would provide the substrate needed for wider clinical validation."