Plain radiographs are a rapid, reproducible, and probably cost-effective technique to diagnose common ligament injuries after wrist trauma, but high-quality images require precise patient positioning, a German study has found.
A Stecher's projection, where the patient closes his or her fist in ulnar deviation, may be mandatory if the primary diagnostic question is ruling in or out an acute scapholunate ligament (SL) tear with all its potential therapeutic consequences, according to researchers from Unfallkrankenhaus Berlin. The SL distance and radiolunate (RL) angle are likely to provide conclusive information for decision-making, and CT or MRI may only be needed in selected cases.
"Plain radiographs remain a highly sensitive and specific primary tool to triage patients with a suspected SL tear to further diagnostic workup and surgical care," noted lead author Dr. Jenny E. Dornberger, from the Department of Plastic Surgery and Burn Care, in an article published online by European Radiology on 17 May. "Reliable threshold values of radiographic indices should prompt further imaging or surgical care. Plain radiographs deliver conclusive clinical information if certain hand positions are used."
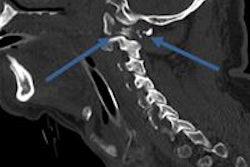
.png?auto=format%2Ccompress&dpr=2&fit=max&q=70&w=700) The width of the scapholunate joint can be measured in the middle of the facet of scaphoid and lunate bones. This method of measuring the SL distance in anteroposterior (AP) projection in neutral radiographs was proposed in Pliefke J et al, Diagnostic accuracy of plain radiographs and cineradiography in diagnosing traumatic scapholunate dissociation, Skeletal Radiol. 2008;37:139-145. Image courtesy of Dr. Jenny E. Dornberger.
The width of the scapholunate joint can be measured in the middle of the facet of scaphoid and lunate bones. This method of measuring the SL distance in anteroposterior (AP) projection in neutral radiographs was proposed in Pliefke J et al, Diagnostic accuracy of plain radiographs and cineradiography in diagnosing traumatic scapholunate dissociation, Skeletal Radiol. 2008;37:139-145. Image courtesy of Dr. Jenny E. Dornberger.Traumatic tears of the SL ligament are the most common ligament injuries of the carpus, typically resulting from forced hypertension or fractures of the wrist, and missed and untreated SL ruptures can cause painful and disabling post-traumatic wrist osteoarthritis, the authors explained. The reported prevalence of SL ligament tears among studies using wrist arthroscopy as a diagnostic reference standard after trauma ranges from 9% to 32%. Clinical red flag signs suggesting a torn SL ligament are persistent tenderness and pain of the SL joint when extending the hand.
"Plain radiographs remain a ubiquitously available and cost-effective clinical standard for the initial diagnostic workup of wrist injuries, and an abundance of measures and indirect signs have been proposed which may signal deterioration of carpal alignment caused by ligament ruptures," they stated. "The best known indices are a widened SL joint space and abnormalities of the carpal angles. Other radiologic features like disruption of carpal arc alignment, a foreshortened scaphoid, loss of SL articular parallelism, or asymmetric widening and a dorsally or subdisplaced scaphoid onto the dorsal rim of the radius in lateral projection have also been associated with this condition and may indicate ligament disruption."
Contralateral radiographs can be a simple reference method for intraindividual comparison of common indices of wrist physiology and pathology. Stress tests may be a useful adjunct to conventional radiographs when screening for SL tears, but research has limited validity because of a retrospective design, convenience sampling, unclear definition of individual signs and quantitative thresholds, and the lack of a consistent reference standard, the author pointed out.
The objective of the Berlin team was to determine the accuracy of common radiological indices for diagnosing ruptures of the SL. Their prospective diagnostic accuracy study involved independent verification of index test findings by wrist arthroscopy. Bilateral digital radiographs in posteroanterior (PA) and lateral views, and Stecher's projection were evaluated by two independent expert readers. Diagnostic accuracy of radiological signs was expressed as sensitivity, specificity, positive predictive value (PPV), and negative predictive values (NPV) with 95% confidence intervals (CI).
Between February 2008 and February 2011, 160 patients were screened for eligibility, and 72 were enrolled in the study (44 men and 28 women with a mean age of 41.4). Forty-five patients had sustained a work-related injury.
Two observers -- a hand surgery resident with five years' experience and a board-certified radiologist with 10 years of experience in interpreting musculoskeletal scans -- independently evaluated all radiographs. Both readers were blinded to surgical reports, and were unaware of the patient's medical history.
The SL distance was measured in neutral PA view, and in the middle of the facet of the scaphoid and lunate (i.e., at the midpoint of the carpal arcs). Carpal angles were measured in true lateral view using the tangential method for the SL angle and axial method for RL angle. The flexed position of the scaphoid was evaluated too.
Arthroscopy of the wrist was performed by two experienced, board-certified hand surgeons. Surgeons were aware of imaging results at the time of arthroscopy. Arthroscopy was performed under general or regional anesthesia. Traction of 3 kg to 5 kg was applied, and standard 3-4, 4-5, 6R, and midcarpal portals were used.
Wrist arthroscopy revealed 27 grade III or IV SL ligament lesions according to Geissler's classification, for an overall prevalence of 38% (95% CI 26–50 %), noted Dornberger et al. The SL distance measured on Stecher's projection proved the most accurate single predictor of SL tears. The area under the receiving operating characteristics curve (AUC/ROCs) obtained by the first and second reader were 92.7% and 90.6%, but both readers experienced difficulties in measuring SL space widening in two cases classified as inconclusive.
Surgery revealed one grade I and IV lesion each. At a cut-off of 3.7 mm, the first reader achieved a sensitivity and specificity of 76.9% and 86.4%, respectively. For the second reader, sensitivity and specificity at this threshold were 80.8% and 84.1%.
"This prospective study confirmed the high accuracy of pathological SL distances and angles but also highlighted the unrivalled importance of the Stecher's projection," they wrote. "Altogether, simple x-ray imaging may deliver conclusive clinical information if certain hand positions are actively used and taken into consideration."
There are limitations of this study, conceded the authors. First, this was a single-center study with fewer than 100 patients and a rather brief period of three weeks of conservative treatment, although this interval resembled clinical practice at other referral centers for hand surgery in Germany. Second, only 45% of all potentially eligible patients were enrolled, suggesting selection bias. Third, the way of performing Stecher's view in this study adhered to reference recommendations but was not standardized in terms of determining the degree of ulnar deviation. Finally, the outcome definition may remain a matter of debate.
"We urge (you) to account for the distribution of values and their likelihood in determining SL ruptures rather than to insist on a single cut-off value when making clinical decisions," they concluded. "We also stress that the physiological variability of the SL joint distance is substantial."