A reconstruction algorithm for CT fluoroscopy demonstrated a "significant" reduction in noise and effective dose compared with filtered back projection (FBP) in a study by German researchers and published online by European Radiology (6 February). The algorithm also boosted readers' confidence.
The group from the radiology and nuclear medicine department at University Hospital Magdeburg in Germany compared image noise, readers' confidence, and effective dose of the reconstruction algorithm with traditional FBP, finding the new algorithm performed better.
Compared with the standard FBP algorithm, the 3D algorithm "yielded a reduction in x-ray tube current while preserving or even reducing image noise, especially in patients with a large body circumference in the imaged region," Dr. Oliver Grosser and colleagues wrote.
Old vs. new
In the last 10 years, minimally invasive procedures performed by CT fluoroscopy became state-of-the-art procedures for different diagnostic and therapeutic interventions, the authors explained. However, despite all the advantages of real-time image guidance during the intervention, CT fluoroscopy is associated with radiation exposure to the patient and subsequent exposure to the interventional radiologist by scattered photons -- particularly in complex interventions.
"Until recently, new reconstruction technologies (e.g., iterative CT reconstructions) were only available for diagnostic CT imaging and for low-dose-applications (e.g., contrast-enhanced CT angiography)," they noted. "Depending on the diagnostic CT application, iterative reconstruction algorithms demonstrated the opportunity for dose reduction of 30% to 75% with preserved image quality."
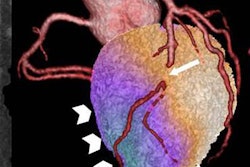
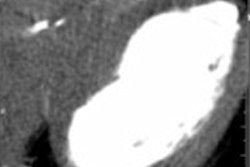
 CT fluoroscopy with FBP (left) and AIDR 3D (right). Body regions were demonstrated in patients with comparable circumferences. Thoracic region: (a) in a patient (female, 73.7 years old, body circumference = 104 cm) for biopsy of a pulmonary lesion and (b) a patient (male, 70.4 years old, body circumference = 108 cm) for drainage placement. Abdominal region: (c) in a patient (female, 50.9 years old, body circumference = 84 cm) for biopsy of a lymph node and (d) a patient (female, 56.1 years old, body circumference = 88 cm) for biopsy of a liver lesion. Pelvic region: (e) in a patient (male, 69.3 years old, body circumference = 98 cm) for biopsy of a lymph node and (f) a patient (male 72.0 years old, body circumference = 94 cm) for drainage placement. All images courtesy of Dr. Oliver Grosser and European Radiology.
CT fluoroscopy with FBP (left) and AIDR 3D (right). Body regions were demonstrated in patients with comparable circumferences. Thoracic region: (a) in a patient (female, 73.7 years old, body circumference = 104 cm) for biopsy of a pulmonary lesion and (b) a patient (male, 70.4 years old, body circumference = 108 cm) for drainage placement. Abdominal region: (c) in a patient (female, 50.9 years old, body circumference = 84 cm) for biopsy of a lymph node and (d) a patient (female, 56.1 years old, body circumference = 88 cm) for biopsy of a liver lesion. Pelvic region: (e) in a patient (male, 69.3 years old, body circumference = 98 cm) for biopsy of a lymph node and (f) a patient (male 72.0 years old, body circumference = 94 cm) for drainage placement. All images courtesy of Dr. Oliver Grosser and European Radiology.Grosser and colleagues used an iterative image reconstruction algorithm (AIDR 3D) to compare how the algorithm fared against the standard image reconstruction, filtered back projection. They included data from 165 patients (FBP = 82) with CT fluoroscopy in the thorax, abdomen, and pelvis. Noise was analyzed in a large-diameter vessel. The impact of reconstruction and variables (e.g., x-ray tube current) influencing noise and effective dose were analyzed by analysis of variance (ANOVA) and a pairwise t-test with Bonferroni-Holm correction. Three readers evaluated noise and readers' confidence.
Noise was significantly influenced by reconstruction, x-ray tube current, body region, and circumference (all p ≤ 0.0002).
AIDR 3D reduced the noise significantly compared with FBP (p = 0.02). The effective dose was influenced by the reconstruction, body region, interventional procedure, and x-ray tube current (all p ≤ 0.02), thus the extent of the effective dose reduction varied for different CT fluoroscopy procedures. Also, patient size (circumference) influenced image noise. For patients with a small body circumference (≤ 100 cm), AIDR 3D had a similar image noise level compared with FBP in interventions of the abdomen and pelvis. However, AIDR 3D had no significant effect in image noise levels in thorax interventions for these patients.
The researchers attribute the effect to the lower attenuation and the a priori low x-ray tube current used in FBP-based CT fluoroscopy in the thoracic region.
The interrater reliability for noise and readers' confidence was good (p < 0.0001). Noise and readers' confidence were significantly better with AIDR 3D than with FBP (p ≤ 0.03).
Limitations
The model-based estimation of the patient exposure represents a limitation of the current study, according to the authors.
"Our analysis used the DLP [dose length product], documented by the CT scanner dose report, to estimate the corresponding effective dose by an established procedure reported by the International Commission on Radiological Protection (ICRP) Publication No. 102," they wrote. "This approach was chosen to reduce the complexity in comparing different scan protocols (e.g., x-ray tube current settings and total scan time) to an estimation of exposure values for the CT fluoroscopy procedure and did not reflect the individual patient's habits."
Another study limitation is the small number of cases and different combinations of interventional procedures in various body regions, meaning the quantity of observations was not sufficient for statistical analysis of the effect of AIDR 3D or FBP in every body region.
Also, the influence of region of interest (ROI) size affects image noise, the authors added.
"From our data, we observed an ROI area approximately two times smaller in the pelvis compared to those of the thorax and abdomen, resulting in an overestimation of the noise level in the pelvis by a factor of √2," they wrote. "This limitation is inherent due to the employed methodology and must be taken into account for the comparison of results between body regions."
Despite the limitations, at Grosser's institution, AIDR 3D is the standard now for CT-guided fluoroscopy interventions.
Because of the small number of cases and the focus on one body region, the authors advocated further studies. In particular, they noted that the effect of dose reductions to staff's exposures should be examined.