Sodium fluoride (NaF) PET/CT provides greater sensitivity and specificity for the detection of bone metastases than planar bone scintigraphy and SPECT/CT, according to a new pilot study from Copenhagen University Hospital.
In the comparison, planar bone scintigraphy also had a relatively high number of equivocal scans compared to NaF-PET/CT, which could reflect uncertainty in reading planar bone scintigraphy due to the modality's low sensitivity and specificity, the researchers concluded.
"Bone scintigraphy is widely used for bone metastases imaging despite its low sensitivity and specificity; that is the reality today," said lead author Dr. Johan Löfgren from the hospital's department of clinical physiology, nuclear medicine, and PET. "But even SPECT/CT is available today and offers 3D SPECT in combination with CT, with evidence of higher sensitivity and specificity compared to planar bone scintigraphy."
Previous studies have shown that NaF-PET/CT finds lesions missed by planar bone scintigraphy and can better differentiate benign from malignant lesions, he said. However, studies have often been small and retrospective, with single-modality PET and without a comparison with SPECT/CT.
Löfgren presented the current study at the recent Society of Nuclear Medicine and Molecular Imaging (SNMMI) annual meeting.
Pilot evaluation
For the ongoing, prospective study, the researchers enrolled 30 patients between June 2012 and April 2013 who were referred for bone scintigraphy with a suspicion of bone metastases. Patients were excluded if they had known bone metastases, were younger than 18 years old, were pregnant or breastfeeding, or had a contraindication to MRI.
Among the study group, 14 patients had breast cancer, 15 had prostate cancer, and one had another form of cancer. The patients had a median age of 59.5 years (± 12.2 years).
Participants were injected with a median dose of 600 MBq of technetium-99m hydroxymethylene diphosphonate (HDP) three to four hours prior to planar scintigraphy, followed by a SPECT/CT scan (Precedence, Philips Healthcare, or Symbia, Siemens Healthcare).
Between two and eight days later, patients were given 200 MBq of sodium fluoride 45 minutes before their PET/CT scan (Biograph True V 40, Siemens), which was followed by PET/MR imaging (Biograph nMR, Siemens).
A nuclear medicine physician and a radiologist who specialized in musculoskeletal MRI interpreted the NaF-PET/MRI results, with MR images serving as the reference standard in case of a discrepancy between planar bone scintigraphy, SPECT/CT, and PET/CT.
An analysis was then conducted on a per-patient basis to determine the presence or absence of bone metastases, with participation from nuclear medicine and CT and musculoskeletal MRI radiologists.
Equivocal scans
Of the 30 patients, five (17%) were found to have bone metastases based on the results from at least two modalities. For 14 patients, there was complete agreement across all modalities, while the remaining 16 had discrepancies.
There were five equivocal scans with planar bone scintigraphy and two equivocal results with SPECT/CT. There were no equivocal scans with PET/CT or PET/MRI.
NaF-PET/CT achieved greater sensitivity, specificity, positive predictive value, and negative predictive value than both planar bone scintigraphy and SPECT/CT, as shown in the table below.
| Comparison of modalities on a per-patient basis | |||||
| Planar bone scintigraphy | SPECT/CT | NaF-PET/CT | |||
| Sensitivity | 60% | 60% | 100% | ||
| Specificity | 56% | 76% | 92% | ||
| Positive predictive value | 21% | 33% | 71% | ||
| Negative predictive value | 88% | 90% | 100% | ||
Given the current focus on radiation dose in nuclear medicine, Löfgren noted that in this study, the dose was approximately 7 mSv for planar bone scintigraphy with SPECT/CT and 8 mSv with PET/CT.
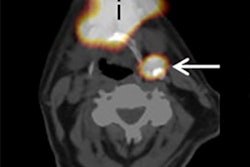
 In this 51-year-old woman with breast cancer, planar scintigraphy shows focal uptake on the rib on the left (ruled an equivocal scan). SPECT/CT shows the same focal uptake in the hip region, which was diagnosed as bone metastases. PET/CT and PET/MRI showed the two lesions but also detected an additional lesion in the midthoracic spine. Images courtesy of Dr. Johan Löfgren.
In this 51-year-old woman with breast cancer, planar scintigraphy shows focal uptake on the rib on the left (ruled an equivocal scan). SPECT/CT shows the same focal uptake in the hip region, which was diagnosed as bone metastases. PET/CT and PET/MRI showed the two lesions but also detected an additional lesion in the midthoracic spine. Images courtesy of Dr. Johan Löfgren.

Based on the results, the pilot study indicates that PET/CT is a "highly sensitive and specific modality" for the detection of bone metastases, Löfgren and colleagues concluded.
"Of course, we need further head-to-head comparisons of bone scintigraphy, SPECT/CT, PET/CT, and PET/MRI and clinical follow-up to help in assessing the consequence of a possible transition from standard bone scintigraphy to NaF-PET-based fusion imaging," Löfgren added. "We hope our study will shed some light on this situation."
When asked why planar bone scintigraphy should even be used, Löfgren did not discount the idea of going straight to SPECT/CT.
"The tradition is planar bone scintigraphy, but today you can do a whole-body SPECT/CT with three bed positions and get a better study than planar [scintigraphy], and it takes 30 minutes to do a whole-body SPECT/CT," he said. "If you want to use the SPECT/CT cameras of today, I think you should skip the planar [scintigraphy] and go to SPECT/CT, where you have CT with increased specificity."