A preliminary study by German researchers suggests that carbon-11 (C-11) choline PET/MRI may provide an alternative imaging modality to PET/CT for restaging of prostate cancer by offering equal, if not better, diagnostic performance and less radiation exposure.
In a comparison between the two hybrid modalities, choline-PET/MRI detected a greater number of suspicious lesions among 31 recurrent prostate cancer patients than PET/CT. However, PET/MRI and PET/CT had similar results in detecting lymph node metastases and bone metastases.
Lead study author Dr. Matthias Eiber from the Institute of Radiology at Technische Universität München, who presented the results at RSNA 2012 in Chicago, said this research is the first clinical experience to compare choline-PET/MRI with PET/CT in the restaging of prostate cancer patients.
"With prostate cancer, there is generally a high rate of recurrence, often after both prostatectomy and radiation therapy," Eiber said. "In these cases, a rise in the PSA [prostate-specific antigen] value usually precedes the clinical detection of recurrence by months and sometimes years."
Physicians in recent years have depended primarily on PET/CT and SPECT/CT to locate prostate cancer recurrence, Eiber noted in his presentation. Past research also has found that choline-PET/CT's detection rates in patients with a PSA value greater than 1.0 is approximately only 40%. Other preliminary studies suggest that PET/CT and whole-body MRI may have additional diagnostic value.
"Whole-body MRI for recurrent prostate cancer has a potential advantage due to the excellence of tissue contrast and also the higher contrast for bone marrow imaging of MRI compared to CT," Eiber added. "There is also the possibility of adding information from functional MRI, such as diffusion-weighted imaging, and dynamic contrast-enhanced imaging due to the tracer uptake in PET."
Imaging protocol
In this study, Eiber and colleagues analyzed 31 patients with recurrent prostate cancer. Each patient had a PSA level of greater than 1.0.
Researchers used a single-injection, dual-image protocol. After the administration of 660 MBq of choline, patients immediately underwent a PET/CT scan. PET/CT was performed on a clinical PET/CT scanner along, with low-dose CT for attenuation correction.
The PET/MRI exam began a mean time of 47 minutes after choline injection and was conducted on a fully integrated system (Biograph mMR, Siemens Healthcare). Patients were imaged from the chest to the pelvis in three or four bed positions, acquiring the PET image four minutes at each position to obtain attenuation correction sequences, coronal T1-weighted spin-echo sequence, and an axial fat-saturated T2-weighted half-Fourier acquisition single-shot turbo spin-echo (HASTE) sequence.
Researchers then proceeded to conduct a 20-minute PET scan over the pelvis to obtain a dedicated MR prostate image in a high-resolution T2-weighted sequence, diffusion-weighted MRI, and a contrast-enhanced imaging sequence.
For image analysis, one nuclear medicine physician and one radiologist independently read the PET/CT and PET/MRI results. All suspicious lesions were rated on a three-point scale, with 1 as definite metastases, 2 as probably metastases, and 3 as an indeterminate lesion.
The researchers also evaluated the scan time for both PET/CT and MRI, and compared the detection rates based on the number of positive findings in anatomical regions. The standard of reference was clinical and imaging follow-up and, in a few cases, histopathology.
Imaging time
In regard to imaging time, PET/CT scans had a mean time of 22 minutes, ranging from 20 to 25 minutes. Choline-PET/MR images lasted a mean time of 43 minutes, ranging from 40 to 55 minutes. Despite a substantially longer imaging time for PET/MRI, the protocol was well tolerated by all patients.
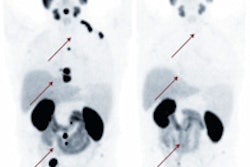
For detecting suspicious lesions in cases of recurrent prostate cancer, PET/MRI found 17 lesions in 11 patients, compared with PET/CT, which detected 11 lesions in seven patients.
The study found a similar performance between the two hybrid modalities for lymph node metastases, with choline-PET/MRI discovering 39 suspicious regions, compared with 38 suspicious regions for PET/CT. In addition, PET/MRI detected bone metastases in 17 regions in five patients, compared with 14 regions in four patients with PET/CT.
PET/MRI also discovered choline-negative, nonsclerotic bone metastases in one patient, which was not identified by PET/CT.
Based on the results, a fully diagnostic PET/MRI protocol with choline for restaging of prostate cancer patients is feasible and well tolerated by all patients, Eiber and colleagues concluded.
The preliminary data found "potentially higher detection rates for local recurrence and only a questionable advantage for bone metastases. For lymph node metastases, there is a similar performance," Eiber added. "Nevertheless, I think studies of this patient collective are promising."
The authors cited some study limitations, including the small number of patients in the analysis. Eiber also noted that, in prostate cancer recurrence, "there is always the question of whether a higher detection rate has a positive benefit on patient outcome."