A muscle injury grading system developed primarily for hamstring problems in elite track and field athletes is gaining clinical acceptance, as evidence emerged at ECR 2015 in Vienna about its reliability.
The British Athletics Muscle Injury Classification (BAMIC) can accurately classify hamstring injuries, which may improve assessment and treatment of injuries, according to Dr. Steven James, specialist consultant musculoskeletal radiologist at the Royal Orthopaedic Hospital in Birmingham, U.K., and colleagues.
Details about the grading system were published online on 26 July 2014 in the British Journal of Sports Medicine. James was one of the authors of this article, along with Dr. Noel Pollock and Dr. Robin Chakraverty, from the British Athletics Medical Team, and Dr. Justin C. Lee, from the department of radiology at Chelsea and Westminster Hospital in London.
"The commonly used muscle injury grading systems based on three grades of injury, representing minor, moderate, and complete injuries to the muscle, are lacking in diagnostic accuracy and provide limited prognostic information to the clinician," they noted.
The authors are convinced the BAMIC provides "a sound diagnostic base for therapeutic decision-making and prognostication." Injuries are graded 0-4 based on MRI features, with grades 1-4 including an additional suffix of "a," "b," or "c" if the injury is myofascial, musculotendinous, or intratendinous. The system offers a diagnostic framework for enhanced clinical decision-making in the management of muscle injuries and assists with future research to inform the development of improved prevention and management strategies, and studies are now underway to validate the classification, they stated in the British Journal of Sports Medicine article.
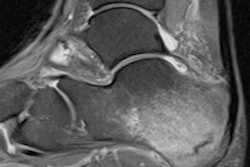
 A 24-year-old male professional football player who presented with sudden onset of pain following striking of the ball. Above: Coronal STIR MRI demonstrates focal defect within the left rectus femoris central muscle at
A 24-year-old male professional football player who presented with sudden onset of pain following striking of the ball. Above: Coronal STIR MRI demonstrates focal defect within the left rectus femoris central muscle at the musculotendinous junction. Note the feathery edema pattern within the muscle radiating from the primary injury site. Below: Extended field-of-view ultrasound demonstrates loculated hematoma at the musculotendinous junction with surrounding increased reflectivity within the rectus femoris muscle. All images courtesy of Dr. Justin Lee, Chelsea and Westminster Hospital.
Muscle injuries are common in sport and result in a significant amount of time lost from training and competition, explained James, who presented an e-poster on the BAMIC at ECR 2015, for which the lead author was Dr. A. Patel. Accurate grading of muscle injuries is important for both clinicians and athletes, and the ultimate goal of an injury classification system is to guide clinical management and provide prognostic information to predict recovery and time off from competition, the authors added.
The most widely used muscle injury grading systems are relatively simplistic, comprising three grades of muscle injury based on imaging findings. Grade 1 represents a strain, grade 2 represents a partial thickness tear, and grade 3 a full thickness tear. But prognostic information on muscle injury is now available based on MRI data like the length of muscle tear, MRI "negative" injuries, distance from the origin of injury, cross-sectional area of edema, and tendon involvement, they noted.
"The old classification systems do not consider the MRI parameters that have demonstrated some prognostic relevance potentially resulting in a number of different injuries (with different treatment and rehabilitation regimens) being categorized into a single group," they continued.
In the ECR e-poster, the authors reviewed 81 MRI scans of elite track and field athletes with suspected hamstring injuries carried out between February 2010 and April 2014. Fifteen of the 81 exams were performed for reasons other than suspected hamstring injury and one was a repeat study. These16 scans were omitted, giving a total of 65 MRI studies from 45 patients available for the analysis.
MRI was performed on different systems at 1.5 or 3 tesla. In most instances, skin markers (cod liver oil capsule) were placed at the site of maximum symptoms. Sequences were dependent on the original institution at which the examination was undertaken, and a typical protocol included a combination of axial, coronal, and sagittal short tau inversion recovery (STIR)/T2-weighted fat-suppressed/proton density-weighted fat-suppressed sequences followed by axial and sagittal T1-weighted sequences. For the study, the images were electronically transferred to a secure electronic database and reviewed using the 32-bit OsiriX DICOM viewer system on the Apple platform.
Two specialist musculoskeletal radiologists independently reviewed all MRI studies and graded the injuries according to the new classification system. All images were reviewed by both radiologists initially (round 1) and again after a four-month period (round 2). When more than one muscle was involved, the muscle with the worst injury was scored. An independent observer, not involved in the study, performed all the statistical analyses.
The team calculated inter- and intrarater reliabilities using the percent agreement and Cohen's kappa statistic. Percentages of agreement were calculated as the number of agreements in observations divided by the total number of observations. Interrater reliability was assessed by comparing the two raters separately for each round and intrarater reliability by comparing each rater's selections from the two rounds.
The BAMIC demonstrated excellent interrater Kappa values of 0.80 (95% confidence interval [CI] 0.67-0.92; p < 0.0001) for round 1 and 0.88 (95% CI = 0.76-1.00; p < 0.0001) for round 2. The percentages of agreement were 85% for round 1 and 91% for round 2. The intrarater Kappa value for the two reviewers were 0.76 (95% CI 0.63-0.88; p < 0.0001) and 0.65 (95% CI 0.53-0.76; p < 0.0001) and the average was 0.71 suggesting substantial overall agreement. The percentages of agreement were 82% and 72%, respectively.
During round 1, there was a discrepancy in the scoring in 10 out of 65 exams, and in round 2, a discrepancy existed in six studies. A third musculoskeletal radiologist reviewed cases where disagreement occurred to give a definitive score. This allowed these cases to be further analyzed to see why differences in opinion about injury grade occurred.
"This study has shown that this classification system is simple to use and produces both reproducible and consistent results based on interobserver and intraobserver reliability with at least substantial agreement in all groups based on calculated kappa values. We believe that as radiologists/clinicians become more familiar with this classification system the inter-rater and intrarater reliability, values are likely to improve," the authors wrote. "Further work is required to investigate how individual grades within this classification system influence clinical management and assist with prognostic information."
French research on footballers
In professional football players, muscle strains usually occur in four main groups of lower limb muscles (37% hamstrings, 23% adductors, 19% quadriceps, 13% calf), according to Dr. Benjamin Coquart, a radiology resident at Hôpital de la Timone, Marseille, who also presented an ECR 2015 e-poster on muscle injuries.
Every muscle has a specific anatomical make-up and structure, which causes a unique lesional spectrum, and knowledge of these aspects can lead to better identification of lesions, he noted. Ultrasound examination must be performed first between the second and the seventh day to avoid underestimating a "fresh" isoechoic lesion. MRI can be added in cases of conflict between clinical and ultrasound findings and suspicion of complete muscular rupture or tendinous avulsion. Standard protocol should include T1-weighted imaging in one section (usually axial) and STIR or T2 with fat saturation-weighted in at least two sections.
"The main benefit of ultrasound is to study muscular contractility and allow imaging-guided treatments (hematoma drainage) at the same time," Coquart stated. "Ultrasonography also allows in most cases to differentiate blurred hyperemic recent injuries (Doppler is classically positive from the third day) from well-defined older injuries. The main asset of MRI is its excellent sensibility, its less operator dependability, and its better deep muscle exploration."