Radiology departments must actively prepare to deal with the COVID-19 crisis because imaging appears set to play an emerging role in the disease, four leading U.K. thoracic specialists have warned in a BMJ blog posted on 12 March.
"Should [RT-polymerase chain reaction (RT-PCR)] results continue to have a prolonged delay (24-48 hours), or be unavailable, the implementation of CT imaging as a frontline diagnostic tool, as rolled-out in China, requires urgent discussion," noted Dr. Samanjit Hare, consultant chest radiologist at the Royal Free London National Health Service (NHS) Foundation Trust, and colleagues.
"A provision for more CT access -- possibly with mobile CT scanners -- may be a step in the right direction," they added.
From a chest radiologist's perspective, however, they fear that without appropriate planning and infrastructure in place for large-volume CT imaging of COVID-19 cases, there are two major risks:
- Potential contamination of scanners, as there may be insufficient time in an already overworked system to provide thorough repeated deep cleaning of machines between CT examinations
- Potential infection of suspected COVID-19 patients who are negative for infection at the time of scanning
"Yet even these concerns do not address the lack of specialist chest radiologists actually required to examine the scans and provide both accurate diagnosis and risk stratification for COVID-19 infected patients," the authors added.
It is also important to bear in mind that CT has only a limited role in diagnosing COVID-19, they continued.
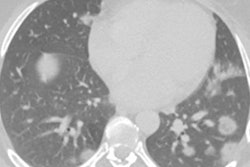
"While CT scanning may pick up abnormalities in the lungs with high sensitivity, the specificity for [COVID-19] diagnosis on CT alone is limited," Hare and colleagues stated.
"Given that changes on CT from [COVID-19] may only appear gradually, it would be prudent to avoid being overly reassured by a normal-appearing early CT in a clinical context suggestive of [COVID-19]," they noted.
Yet there are scenarios where CT may be required earlier in the diagnostic pathway, and in spite of the modality's limitations, radiology departments must remain ready to answer the call, they wrote.
"The primary advantage of CT imaging is its speed of diagnosis. Yet even when CT is available, the current lack of specialist chest radiologists in the U.K. may provide a barrier to timely diagnosis of [COVID-19], particularly when findings are subtle (seen in early disease) and/or atypical," the authors pointed out.
As a crisis point approaches, radiologists need to start planning now whilst putting aside the deep-seated frustration held by U.K. radiologists who have consistently argued about the need for greater radiology investment, they concluded.
Hare's co-authors are Dr. Joseph Jacob, from University College London; Dr. Annette Johnstone, from Leeds Teaching Hospital NHS Trust; and Dr. Graham Robinson, from Royal United Bath Hospitals Bath NHS Foundation Trust. All four authors are committee members of the British Society of Thoracic Imaging.




COVID-19_FDG_PET_CT_JNM_Albano_Image_G_400.png?auto=format%2Ccompress&fit=crop&h=167&q=70&w=250)












