CT lung cancer screening is at the fore with 10 new recommendations from the European Society of Thoracic Surgery (ESTS). A recently published paper written by an international team of eight experts in the field of thoracic surgery outlines the ESTS's plans for improving lung cancer CT screening by involving surgeons at all levels of screening strategy.
The paper, "Recommendations from the European Society of Thoracic Surgeons (ESTS) regarding computed tomography screening for lung cancer in Europe" was published online on 30 January in the European Journal of Cardio-Thoracic Surgery.
The 10 recommendations straddle six key areas, according to the author group. These areas include the following:
- Implementation of CT screening in Europe
- Multidisciplinary capabilities and requirements for screening centers and diagnostic protocols
- Participation of thoracic surgeons in CT screening programs
- Training and clinical profile for surgeons participating in screening programs
- Use of minimally invasive thoracic surgery and other relevant surgical issues
- Incorporation of associated elements of CT screening programs (i.e., smoking cessation programs, radiological interpretation, nodule evaluation algorithms, and pathology reports)
ESTS aims to provide guidance and facilitate the growing involvement of surgeons in the screening process, according to lead author Dr. Jesper Pedersen, chief surgeon in the department of thoracic surgery at Rigshospitalet, University of Copenhagen.
 Dr. Jesper Pedersen, chief surgeon department of thoracic surgery at Rigshospitalet, University of Copenhagen.
Dr. Jesper Pedersen, chief surgeon department of thoracic surgery at Rigshospitalet, University of Copenhagen."The recommendations are important because surgeons will play a key role in the planning and implementation of CT screening in Europe. Most of the nodules detected during screening will require evaluation by cardiothoracic surgeons, and it is extremely important that surgeons prepare for this task, which is very different from the clinical situation with symptom-detected lung cancer," Pedersen told AuntMinnieEurope.com. "CT screening will require very close collaboration between surgeons and radiologists, but should not be the cause of conflicts if the screening protocols are well prepared and agreed on at multidisciplinary team (MDT) conferences. The joint commitment to the screening process and the safety of the screened persons require that all specialists participate and contribute."
According to the paper, around 269,000 deaths in Europe from lung cancer were expected in 2016. The authors believe it is clear that screening and early detection can contribute to reducing lung cancer mortality. They also pointed to CT screening being recommended in a white paper by the European Society of Radiology (ESR) and the European Respiratory Society (ERS).
The ESTS' 10 proposals are based on the likely scenario that, in Europe, CT screening for lung cancer will have to be implemented within the next few years. In the first recommendation about implementation in Europe, ESTS envisages that each country makes preparations to facilitate the process according to specific cultural, political andsocioeconomic circumstances.
Smaller countries may partner with larger bordering countries or international organizations, while countries with previous or ongoing screening experience may develop demonstration programs as well as joint protocols between different local screening centers for national implementation. The paper also calls on financial support from the European Union (EU) under the banner of the EU research fund, Horizon 2020.
The second recommendation specifies the involvement of thoracic surgeons in preparation, structuring, and implementation of screening programs.
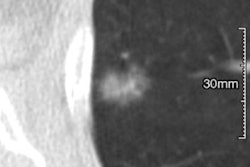
 CT screening detected a part-solid ground-glass opacity nodule from the Danish Lung Cancer Screening Trial. Final diagnosis was adenocarcinoma. All images courtesy of Dr. Jesper Pedersen.
CT screening detected a part-solid ground-glass opacity nodule from the Danish Lung Cancer Screening Trial. Final diagnosis was adenocarcinoma. All images courtesy of Dr. Jesper Pedersen."With the increasing rate of detection of early lung cancer through screening [low-dose CT] LDCTs, surgeons will be called to provide the necessary expertise to obtain both diagnosis and treatment of screen-detected nodules," the authors stated.
The paper referred to high-quality lung cancer screening programs in the U.S., in which the surgeon plays a leading role within the lung cancer screening MDT, and listed the major goals of surgical participation in lung cancer screening as follows:
- Optimization of the management of screen-detected nodules
- Reduction of false-positive rates of surgical biopsies
- Reduction of surgical incision-related trauma
- Implementation of national or international risk assessment guidelines
- Implementation of a smoking cessation policy
- Active education of primary care physicians toward lung cancer screening programs
How will radiology respond to the paper? At least one senior thoracic radiologist was skeptical.
"It is not very specific. There are no obvious conflicts with regard to what the ERS or ESR recommended," he said. "It is clear that thoracic surgeons want to be part of the game, although they cannot and do not overrule current knowledge and processes regarding management of small nodules."